INTRODUCTION
Peripheral neuropathy refers to sensory/motor neuropathy with pain, and it is a major complication that occurs in approximately 40% of cancer patients who receive chemotherapy [1]. Anticancer drugs such as vinca alkaloids, taxanes, and platinum agents are frequently associated with sensory neuropathic symptoms, such as tingling and numbness, as well as motor neuropathic symptoms that may be the cause of muscle weakness and some difficulty in walking [2,3]. Approximately 20% of cancer patients receiving concomitant chemotherapy complain of urinary retention or residual neuropathy [4,5].
Lower urinary tract symptoms (LUTS) include dysuria and motor and sensory nerve dysfunction in the urethra. LUTS are divided into storage symptoms, such as frequency, nocturia, and urinary incontinence; voiding symptoms, such as hesitancy and straining; and post-voiding symptoms, such as residual urine sensation and postvoid dribbling [6]. A previous study reported that more than 70% of patients who received chemotherapy complained of LUTS, and LUTS may continue for months or even several years after chemotherapy [7,8]. LUTS have been associated with cancer treatment methods and the duration of disease after cancer diagnosis [8]. It has been reported that 68% of patients receiving chemotherapy complained of nocturia [9], and that 37.0% of cancer survivors showed urinary incontinence, but only 19.2% of them had received treatment [10].
Radiotherapy can irritate the bladder wall lining and muscle wall, leading to decreased bladder compliance and capacity [11]. Furthermore, chemotherapeutic drugs such as paclitaxel/carboplatin therapy and cyclophosphamide can cause chemical-induced hemorrhagic cystitis symptoms (e.g., frequency, urgency, and pelvic pain) [12], which can increase the risk of cystitis, fibrosis, sphincter dysfunction, or bladder muscle stiffness [11,12]. As LUTS in advanced cancer patients can be a main reason for diminished quality of life (QoL), continuous management is necessary [7].
Limited studies have been conducted on LUTS-associated factors and QoL [8] and voiding dysfunction after cancer surgery [13]. This study aimed to investigate LUTS severity, to identify the factors that influenced LUTS in advanced cancer patients with chemotherapy-induced peripheral neuropathy (CIPN), and to provide baseline data for the development of nursing interventions aiming to improve micturition-related QoL.
MATERIALS AND METHODS
Study Design
This was a cross-sectional study designed to investigate the severity of LUTS and factors that influenced LUTS in advanced cancer patients with CIPN.
Participants and Data Collection
The participants in this study comprised 158 advanced cancer patients admitted to the Oncology Department in St. Mary’s Hospital, The Catholic University of Korea, Seoul, South Korea. Participants agreed voluntarily to participate in this study after being informed about its purpose and procedures, and convenience sampling was used to recruit the sample of 158 participants.
The selection criteria included persons 18 years or older with stage III/IV gastric or lung cancer who had been treated with chemotherapy (>at least 1 cycle of platinum and/or taxane compound agents at the oncology clinic), had no preexisting CIPN symptoms prior to initial chemotherapy, and were classified as National Cancer Institute-Common Toxicity Criteria (NCI-CTC) grade I or higher.
Data collection was conducted from February 2014 to June 2014, and the study received approval from the Institutional Review Board of St. Mary’s Hospital, The Catholic University of Korea (KCI13OISI0345). Patients who met the selection criteria were informed about the purpose, methods, and procedures of the study, as well as about how to withdraw from participation. Written consent was obtained from patients who agreed to participate in the study. One researcher screened and selected grade I or higher patients based on the NCI-CTC grading system of peripheral neuropathy.
Instruments
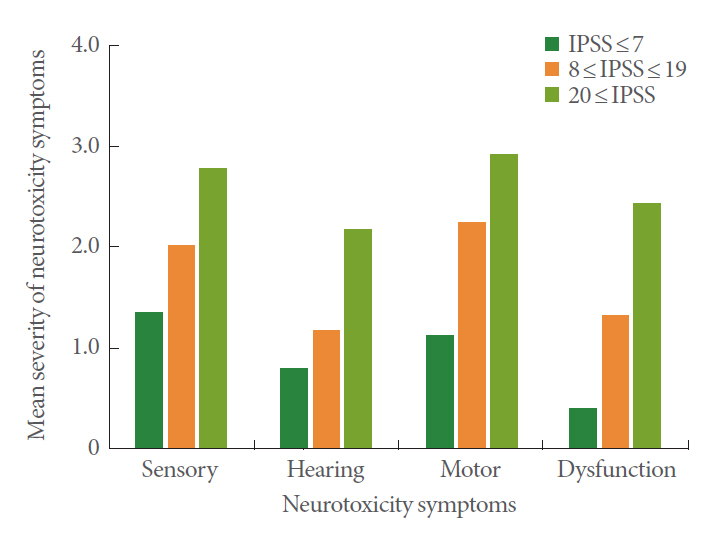
Information about demographic and clinical characteristics was collected using self-reported measures and medical chart review. Peripheral neuropathy symptoms were measured using the neurotoxicity subscale of the Functional Assessment of Cancer Therapy/Gynecology Oncology Group/Neurotoxicity scale [14]. This tool comprised a total of 11 items pertaining to sensory, hearing, motor, and dysfunction symptoms. Each item was rated on a 5-point Likert scale (0–4), with a higher score indicating more severe symptoms.
LUTS were measured based on the International Prostate Symptom Score (IPSS) originally developed by Barry et al. [15] and translated into Korean by Choi et al. [16]. This tool consisted of 7 LUTS and IPSS-QoL measures associated with micturition. The severity of each LUTS level was rated on a 6-point scale (0–5), and the IPSS-QoL was rated on a 7-point scale (0–6). The severity of LUTS was classified into 3 grades: mild (0–7 points), moderate (8–19 points), and severe (20–35 points). Thus, higher IPSS-QoL scores indicated lower micturition-related QoL.
Statistical Analysis
All collected data were analyzed using SAS ver. 9.2 (SAS Institute Inc., Cary, NC, USA). The general characteristics of the participants and LUTS severity were analyzed and presented as frequency, percentage, mean, and standard deviation. Differences in LUTS according to participants’ general characteristics were analyzed through the t-test and analysis of variance. Correlations between CIPN symptoms and LUTS were analyzed using the Pearson correlation coefficient. Factors influencing LUTS were analyzed through multiple regression analysis.
RESULTS
Participants’ General Characteristics
The mean age of the participants was 61.3 years and 60.1% of them were male. Those with a body mass index of less than 23 kg/m2 accounted for 53.2% of all participants, and those with an Eastern Cooperative Oncology Group (ECOG) score of 2 points accounted for 48.1%. Additionally, 24.7% of the participants had gastric cancer, 75.3% had lung cancer, and 86.1% had stage IV cancer. The mean length of time after cancer diagnosis was 24.9 months, and 70.9% of participants did not receive any surgical treatment for cancer. The mean length of time after initial chemotherapy was 17.4 months. Of the participants, 64.6% were classified as NCI-CTC grade II, and 49.4% were treated with concomitant platinum and taxane chemotherapy. The mean number of cycles of platinum or taxane chemotherapy was 9.9 (Table 1).
Severity of CIPN and LUTS
The mean score for CIPN symptoms was 20.17 points. The mean score for LUTS was 14.15 points. The mean score for voiding symptoms was 7.85 points, and the mean score for storage symptoms was 6.37 points. Nocturia (2.67 points) was the most severe symptom, followed by weak urinary flow (2.39 points) and straining (2.11 points). The average IPSS-QoL score was 3.15 points (Table 2). Twenty-five participants (16.5%) had mild LUTS, 100 (63.3%) had moderate LUTS, and 32 (20.2%) had severe LUTS (Table 3).
Relationship Between LUTS and CIPN Symptoms
There was a moderate positive relationship between CIPN symptoms and LUTS (r=0.53, P<0.001). In other words, severe CIPN symptoms were associated with severe LUTS (Fig. 1).
Differences in LUTS According to the Participants’ General Characteristics
Differences were found in LUTS according to age, ECOG score, diagnosis, the length of time after cancer diagnosis, the length of time after initial chemotherapy, and NCI-CTC grade (Table 1).
Factors Influencing LUTS
This study investigated various factors that were related with LUTS, such as general characteristics, ECOG score, diagnosis, the length of time after cancer diagnosis, the length of time after initial chemotherapy, the length of time after the onset of CIPN symptoms, and the severity of CIPN symptoms. All these factors were analyzed as independent variables, and there was no issue of multicollinearity among these variables.
The regression model for LUTS showed a significant relationship (F=10.20, P<0.001), with an explanatory power of 40%. The length of time after cancer diagnosis and the severity of CIPN symptoms were the main factors that significantly influenced LUTS. The severity of CIPN symptoms was the most influential factor (Table 4).
DISCUSSION
The present study investigated LUTS and factors influencing LUTS in advanced cancer patients with CIPN symptoms. The mean LUTS score was 14.15 points (out of 35 points), indicating moderate severity. This score was higher than the LUTS score in patients with invasive bladder cancer (between 6.6 and 7.1 points) reported in a previous study [8] and the LUTS score for rectal cancer patients receiving chemotherapy (6.2 points) reported by Kim et al. [17].
In this study, 16.5% of advanced cancer patients with CIPN had mild LUTS, 63.3% had moderate LUTS, and 20.2% had severe LUTS. This finding shows a trend for a higher proportion of moderate and severe LUTS than was found in advanced prostate cancer patients receiving brachytherapy (mild, 50.0%; moderate, 39.0%; and severe, 6.0%) [18]. In this study, the IPSS-QoL score and the micturition-associated QoL score were 3.15 of 6 possible points, which was higher than the score for IPSS-QoL (2.7 points) in rectal cancer patients following rectal resection with autonomic nerve preservation [17]. LUTS have been found to negatively influence the QoL of cancer patients [8].
In the present study, LUTS severity was positively related to CIPN symptoms. No previous studies have investigated the relationship between LUTS and CIPN symptoms; therefore, it was not possible to compare the results of this study to those of other previous studies. However, the study of cervical cancer patients by Benedetti-Panici [19] reported that LUTS such as sensory loss, difficult micturition, and severe urinary incontinence occurred in 26% of cervical cancer patients after 12 months of treatment with platinum anticancer drugs. Stubblefield et al. [5] considered that areflexia, LUTS such as urinary retention, and CIPN symptoms might occur after the administration of anticancer drugs such as platinum and paclitaxel, indirectly suggesting that CIPN symptoms may be relevant to LUTS. However, the present study was conducted using a subjective self-administered questionnaire; therefore, it had a limited capability to identify objective causality. Further studies using objective measurements are needed to clarify the causality.
In the present study, LUTS increased in severity with age, and it can be assumed that the aging process of the body may decrease bladder muscle tension and increase bladder volume or the sensation of residual urine, resulting in more severe LUTS; thus, the prevalence of storage LUTS and voiding LUTS such as frequency and nocturia increases with age [20,21]. In addition, older patients may have an increased incidence of adverse effects associated with chemotherapy, as well as a decreased ability to cope with them [22]. Therefore, attention should be paid not only to the severity of LUTS, but also to the cause and subsequent effects of LUTS in elderly cancer patients. In particular, the relationships of older age and male sex with the severity of LUTS should be analyzed.
Even though the present study found no sex-related differences in LUTS, previous reports have found that males had more severe LUTS than females [23,24]; further studies of the effect of sex on the relationship between CIPN symptoms and LUTS severity are therefore warranted.
A higher ECOG score in advanced cancer patients was associated with more severe LUTS. Gift et al. [9] reported that because cancer patients perceived greater weakness, fatigue, and physical limitations than other patients, they complained more of nocturia symptoms. A decrease in physical activity was reported to be a risk factor for the onset of LUTS [25]. Study participants with NCI-CTC grade II/III CIPN symptoms were found to have severe LUTS. Individuals with an NCI-CTC grade II/III have impaired daily life activities or severe functional impairment due to sensory loss or paresthesia [26]. It can be assumed that, in NCI-CTC grade II/III patients, the bladder becomes rigid or contracted, thereby leading to the development of symptoms such as nocturia and straining while voiding.
In the present study, longer lengths of time following cancer diagnosis and initial chemotherapy were associated with more severe LUTS. This tendency likely occurred because advanced cancer patients had been repeatedly administered neurotoxic anticancer agents such as taxane or platinum compounds for the treatment of invasive sites. The severity of CIPN symptoms increased as the number of administered doses increased [5,26]. Long-term administration of oxaliplatin or cisplatin might lead to sympathetic and parasympathetic nervous system dysfunction, and has been found to result in urogenital dysfunction [27]. Additionally, a previous study reported that the cumulative dose of paclitaxel or docetaxel was closely clinically related with the degree of chemotherapy-related peripheral neurotoxicity, and that cumulative doses in line with treatment progression were accompanied by motor or autonomic impairment [28]. However, the length of time after the last chemotherapy session and the number of chemotherapy cycles were not investigated in this study. Cumulative or nerve damage and a short interval after chemotherapy might aggravate voiding dysfunction. Further studies are required to determine the effects of the cumulative dose of anticancer agents on LUTS.
Multiple regression analysis was performed to investigate the factors influencing LUTS in advanced cancer patients with CIPN symptoms. The length of time following cancer diagnosis and the severity of CIPN symptoms were found to be key factors influencing LUTS, and the severity of CIPN symptoms showed the greatest influence. Windebank and Grisold [27] stated that the length of chemotherapy treatment and preexisting neuropathy influenced the development and the severity of CIPN, and autonomic dysfunction or urogenital dysfunction of the urinary bladder occurred in patients receiving long-term administration of neurotoxic anticancer agents such as oxaliplatin or vincristine. Cancer patients with LUTS may have a reduced QoL because they are more restricted in their physical functions and social roles than those without LUTS [8]. Therefore, continuous assessment and management of LUTS, as well as CIPN symptoms, are important for advanced cancer patients even after treatment.
This study investigated LUTS in advanced gastric and lung cancer patients with concurrent CIPN symptoms; therefore, these results cannot be generalized to all cancer patients. As such, further studies are required to expand the scope of participants to include advanced solid cancer patients with CIPN symptoms, such as patients with metastatic colon, breast, or ovarian cancer [4] and to investigate the relationship between CIPN symptoms and LUTS. In addition, studies should consider not only the length of time after cancer diagnosis, but also the duration of the cancer stage related to LUTS.
This study had a limitation in that it did not identify alpha-blockers or anticholinergics, which may influence bladder function, among the drugs administered to cancer patients. This study included a relatively large sample of male patients who were older than 60, and therefore could have been vulnerable to selection bias. This was a cross-sectional study; thus, it would be difficult to compare IPSS scores before and after chemotherapy.
Another limitation of this study is that it did not extensively consider the various comorbid conditions that can affect LUTS. Such conditions include arthritis, asthma, depression, diabetes, heart disease, neurological conditions, and recurrent urinary tract infections [29]. Further studies are needed of the effect of general status or performance in addition to the ECOG score. The prevalence of LUTS may increase in patients with symptoms of depression [23]; therefore, studies on the effects of LUTS on comorbid conditions and psychological variables may be worthwhile.
In conclusion, nocturia was found to be the most prevalent LUTS in advanced cancer patients experiencing CIPN. The length of time after cancer diagnosis and the severity of CIPN were found to be factors influencing LUTS. In particular, the severity of CIPN symptoms was the most important predictor of LUTS.
Therefore, patients’ urination status should be considered before initiating treatment with anticancer drugs that can cause CIPN. We suggest that nurses caring for advanced cancer patients should conduct a comprehensive health assessment that includes a history of treatment, physical neuropathic symptoms and severity, mobility, daily life activities, and LUTS, for any patient complaining of CIPN symptoms. In practice, it is necessary to develop micturition-related nursing assessment records and nursing intervention algorithms, and to provide CIPN information and education regarding LUTS management to the relevant patients prior to initiation of chemotherapy.