Virtual Reality and Simulation for Progressive Treatments in Urology
Article information

Abstract
In urology technologies and surgical practices are constantly evolving and virtual reality (VR) simulation has become a significant supplement to existing urology methods in the training curricula of urologists. However, new developments in urology also require training and simulation for a wider application. In order to achieve this VR and simulation could play a central role. The purpose of this article is a review of the principal applications for VR and simulation in the field of urology education and to demonstrate the potential for the propagation of new progressive treatments. Two different cases are presented as examples: exposure therapy for paruresis and virtual cystoscopy for diagnosis and surgery of bladder cancer. The article uses research and publications listed in openly accessible directories and is organized into 3 sections: The first section covers features of VR and simulation technologies. The second one presents confirmed applications of current technologies in urology education and showcases example future applications in the domain of bladder treatment and surgery. The final section discusses the potential of the technology to improve health care quality.
INTRODUCTION
In medicine in general and in the field of urology in particular, the traditional way of education and apprenticeship is evolving with times and technology. The conventional method of teaching surgery by “see one, do one, teach one” has radically changed with new technologies [1]. Simulations have become a constant element of education and training - as well as augmented (AR) and virtual reality (VR). The origin of these terms emerges from the research on mixed reality [2] where AR describes a real environment enhanced with artificial and computer generated imagery, and VR describes the substitution of a real environment by artificial and computer-generated imagery. These virtual environments are accomplished by the means of displays inside headsets known as head mounted displays (HMDs). The term simulation is often used as a synonym and refers to an “artificial representation of a real world process” [3]. It generally includes accurate haptic interaction as compared to AR and VR, which mainly focus on visual simulation.
Since 2016, a new movement of VR and AR has emerged with a new generation of devices deployed on the consumer market. Mainstream media and research institutes forecast a large growth for VR and AR in the medical and health care sector. This market segment could reach up to USD 285 million by the year 2020 [4]. Researchers and manufacturers predict large opportunities in education, in medicine in general and in the field of urology in particular [5]. An increase in scientific publications on the subject of VR and AR can be observed [6] over the same period of time.
The profession of urology is traditionally open to new technologies and methods. It places itself at the forefront of robotic and minimally invasive surgery, and it has a particular demand for training and education of additional learning skills [7,8]. Urology requires skills in many different disciplines and most curricula take into account that not only technical, but also nontechnical skills such as teamwork, crisis-management and leadership are crucial. All these aspects are necessary and require adapted training technologies and teaching methods.
Training in real situations is often not possible, due to reasons of costs and/or danger. At the same time a constantly increasing demand and level of quality in health care makes it necessary that urologist residents and trainees acquire as many skills and experiences as possible, also outside of the operating room. This is why VR and simulations are constantly gaining importance and they have become crucial when it comes to the training of new methods and practices.
The purpose of this review article it to provide an overview of the current applications of these new technologies and to show how they can be adapted for the introduction and propagation of new treatments and surgery methods. The review of the contemporary VR and AR applications is based on research available in the scientific publication directories Springer, Google Scholar, IEEE, PubMed, and Elsevier. The referenced research is not exhaustive, but can highlight trends in a specific field of application.
This article is organized into 3 sections: The first section introduces the technologies used in VR and simulation. The second section reviews exemplary VR applications [9] in the field of contemporary urology education and demonstrates how these technologies can be used in training and propagation of progressive methods using examples of bladder treatment and surgery. The final part draws a conclusion and outlines how development of the technology can be used to improve professional skills for urologists and the quality of health care for patients.
VIRTUAL REALITY TECHNOLOGY
The field of VR and simulation covers many different types. The most important and commonly used technologies are presented in this section with their features and limitations: ubiquitous, immersive, interactive, haptic, and augmented systems.
Ubiquitous Systems
One of the simplest and vastly used virtual training systems is Elearning. They represent a ubiquitous source of learning materials and courses which can be accessed from anywhere at any time and can therefore be considered virtual classrooms. Knowledge and lectures can be accessed without instructors and assessments are easily implemented. They can be part of a curriculum as an online extension of a university or urology education institution or they can be a service offered by the different associations in the urology sector with the aim of promoting new technologies and practices available to their members and urologists all over the world. An example is the web presence of the European Association of Urology. It not only contains a lot of information about urology, research and news about the profession, but also an important educational section with urology education material such as presentations, videos and E-Learning resources[10].
Although great advantages such as the ease of access and the broad field of subjects that can be covered, the E-learning systems have obvious limitations: Even with conventional videos and text, the implication of the user and learner is restricted to theory. The technology simulates learning, but not the actual procedure and action necessary in urology.
Immersive Systems
The theoretical aspect and the lack of immersion of the previous technology can be overcome by the usage of VR360 degree videos. These panoramic movies represent immersive VR experiences. They are recorded with omni-directional cameras either in stereoscopic 3-dimensional (3D) or 2-dimensional. The videos are usually watched using VR headsets or HMDs. These exist in 2 variations: the first is a fully dedicated device. This technology has seen a break through on the consumer market in recent years and the main manufacturers of this immersive VR are Oculus Rift and HTC Vive [11]. This technology requires powerful hardware. Motion capture sensors around the headset communicate position and viewing angle to a computer. A dedicated software reproduces a matching viewpoint and gives the user the feeling of taking part in an interactive environment. The second variation is an often more affordable solution for presenting VR360 videos: It consists of a smart phone in combination with a cardboard type HMD. The sensors in the smart phone are used to calculate the appropriate viewing angle for the user. Recent research has shown that both variations of this technology provide similar learning results, however content on mobile based HMDs is recommended to be shorter than desktop-based systems, due to higher risk of motion sickness that can occur during the viewing [12]. Two applications of this immersive technology are worth mentioning: One in the field of educational promotion, the other in the domain of immersive urological training videos.
In 2016, the Italian Society of Urology organized the Italian urology conference iTrust16. Its subject was education and simulation in urology. Among other media, it used VR360 videos for Internet communication and sharing conference highlights on YouTube [13]. In the United States, a web-based service and community, GIBLIB, aims to index every possible surgical procedure and also offers access to a variety of VR360 videos of urology surgery [12,14].
The VR360 technology has the advantage of setting the user in an immersive environment, The user can simulate the situation of a surgery in an environment where access is usually difficult. The panoramic view allows a realistic orientation in the virtual environment. However, this technology has a limitation, it lacks interaction. Training of action in dedicated situations is limited.
Interactive Systems
Virtual labs are dedicated game like computer programs that simulate handling and physics in a certain environment. They are often used on laptops and class room screens when a real lab is too costly or not available. Virtual labs take advantage of the performance of modern computers in combination with powerful GPUs. Virtual labs are generally used in undergraduate education and in institutions which teach many students and do not have the equipment available e.g., to perform large scale chemical, biotechnology or physics experiments. Students can perform tutorials and exercises like a game on their web browsers. Assessment of the courses is done inside the lesson sessions. Studies have shown that such gamified simulations in virtual labs can improve education [15,16]. The Indian company, labOnLaptop (Gujarat, India), has developed a game like platform for urology education with a virtual operation theater as shown in Fig. 1.
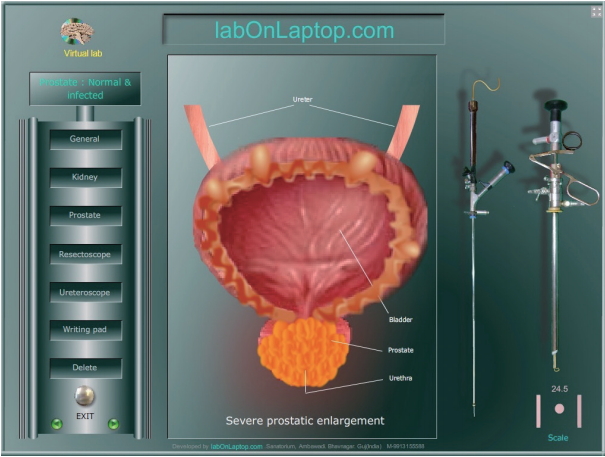
Lab on Laptop: urology, simulated operation theater.
The virtual lab does not provide the level of immersion as in the VR360 videos, but allows game-like interaction for practice of several urology intervention scenarios [17,18]. However, even if the scenarios are realistic, the intervention itself remains mainly theoretical, since it lacks a very important feature: haptic simulation.
Haptic Systems
Accurate and precise simulations are usually provided by devices referred to as box simulators or bench top simulators. They consist of dedicated devices that aim at accurately and precisely reproducing anatomic and haptic environments of the procedure to simulate. Urologist surgeons need training with simulators in order to get familiar for example with the particular laparoscopic and endoscopic skills. The use of simulators helps urologist surgeons to improve their skills and to acquire more experience outside of the often dangerous and costly environment of the operating room.
A recent example can be also observed in the programmable pneumatic prostate palpation simulator. This new device allows the urologist apprentice to practice the detection of various diseases with realistic haptic feedback. The simulator provides high level haptic realism and can generate multiple stages of anomalies for training [19].
The simulators undergo a validation of their realism and accuracy, however in box simulators a problem remains: how can assessments be performed? Such assessments need to come from an experienced urologist or a complex validated training software attached to the simulator.
Augmented Systems
Another way to overcome the lack of haptic realism is the use a real environment enhanced by additional visual information. This is the principle of training with AR. One recent example is the HMD manufactured by Microsoft under the name of Holo-Lens. This device allows seeing a real environment while watching overlayed computer generated elements realistically positioned in space using modern motion sensors and tracking. The first medical example application was announced in 2016 by a joint project of Case Western University in cooperation with Microsoft [20]. In a special showcase Microsoft demonstrated the possibility of displaying 3D models in space and how to manipulate their position and size with gestures. The possibility to move around virtual objects was presented as a big advantage in the learning process of human anatomy. Fig. 2 shows the AR demonstration of a urology anatomy education application [21].
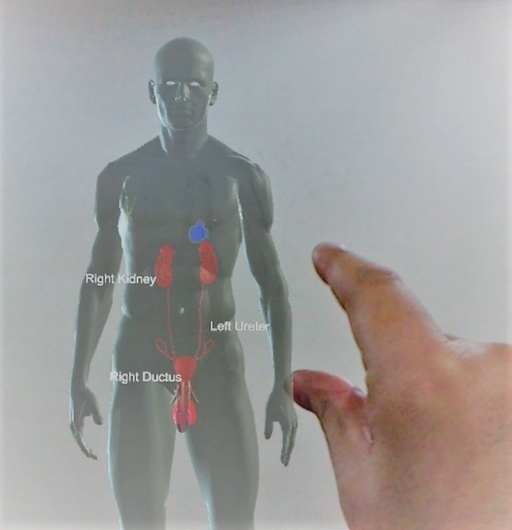
Urology anatomy with HoloLens, augmented reality application.
While the overlapping of virtual 3D models over real environments is one particularity of AR applications with headsets such as HoloLens, it is not the only method to create AR experiences. By creating specific software interfaces inside their operating systems companies like Apple and Google have implemented libraries for the development of AR content on mobile devices such as smart phones or tablets. The key technology is similar in many cases: It allows tracking objects and markers and displaying virtual images and objects as an overlay of the live images taken by the internal camera of the mobile device. Apple calls this technology AR-Kit, Google names it AR-Core. Both technologies allow simulating a see-through experience and creating AR experiences for the user.
These technologies can be used for example to overlap computed tomographic scan images over body parts or to display additional information during surgery. Experiments have been made to show that such supplemental information displayed in AR applications can be useful in certain cases and compensate for the loss of haptic sensations such as in robotic or telesurgery [22].
COMPARISON OVERVIEW
Different technologies represent different advantages and limitations. Each can have their dedicated field of applications. Table 1 shows that there are also a few overlapping features in each technology. In order to overcome the limitations, modern systems tend to evolve and it is likely that future systems will combine multiple technologies in order to provide realistic virtual environments together with meaningful feedback and assessments.
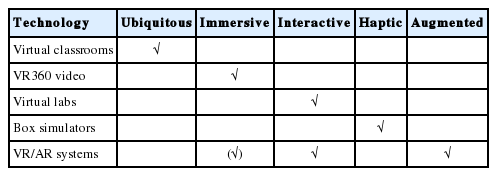
Overview simulation technologies
Training with simulators is uncontested and studies show that VR simulations contribute to improved performance in the operating room [23]. Brunckhorst et al. [24] published a broad overview of available urological simulation technologies and also compared benchmarks for different simulations. Table 1 shows a summarized version of this simulation overview. The table shows the increasing number of VR based simulations available for urology.
Many of these simulations are already part of urological education curricula, either in frameworks for urological training programs or dedicated hands-on workshops. The following section reviews how these technologies are applied in the teaching of present and new urology practices. This section consists of 2 parts: The first part is dedicated to specific simulation and VR applications in proven urology education. The second part will show the examples of 2 new types of applications in the field of bladder related treatment and surgery.
VIRTUAL REALITY AND SIMULATION IN UROLOGY EDUCATION
A large diversity of educational AR and VR applications in urology can be observed in different types of applications, hardware and software. They are usually all developed for a specific target and adapted to one dedicated focus in urology education. During their education the future urologists have to acquire broad knowledge and progressively develop the skills necessary for the profession.
Instruction of doctors, medical staff and team members is the central part of urology education. This section shows the confirmed applications in urology education, in 3 major fields: Theoretical knowledge, technical as well as nontechnical skills.
KNOWLEDGE
One of the primary knowledge requirements in medicine is the mastering of anatomy. It is one of the first applications for AR that was published as demo by Microsoft immediately when the first HoloLens HMD was released in 2016 [20]. While a lot of the gross anatomy education is still done on cadaver dissection, because it has a long tradition in medicine, little evidence exists to evaluate the performance of this learning method [25]. AR and VR can have a place in anatomy education.
NONTECHNICAL SKILLS
One of the main reasons for the necessity of nontechnical skills is the simple fact, that urologists usually do not work alone. They are often surrounded by a team of other doctors and experts, nurses and medical staff. Working efficiently and well in a team is a major key to success. Such nontechnical soft skills are often important for the outcome of many interventions, and they are crucial in emergency situations.
In the United Kingdom (UK), a recently introduced boot camp for aspiring urologists has included the training of non-technical skills in the curriculum [26]. The aim is not only to teach technical skills through simulations, but also the teaching of professionalism and nontechnical skills such as judgment, decision-making, teamwork, and communication. This boot camp addressed these points using efficient time management, talks on professionalism and medico-legal talks as well as discussions about human factors to consider. A significant outcome of this kind of boot camp, which was the first in its kind offered in 2017, was the increase in confidence among urologist trainees. Assessment of this particular training method was made through numerous questionnaires before and after the training sessions in order to evaluate the individual training modules.
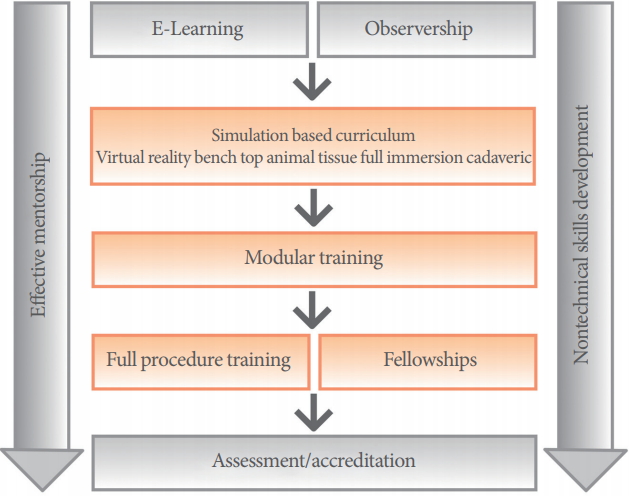
Fig. 3 shows the proposition of a framework using simulation inside the curriculum of urological training programs in the UK. It describes the different types of simulation techniques and organizes them by the stages of the training program. It displays technical and nontechnical skills and recommendations for appropriate simulation methods. The proposed simulation techniques for nontechnical skills such as decision-making and communication are paper scenarios, classroom teaching and role-playing. These are to be applied in an early stage of the urological training program. In an intermediate stage, leadership and stress management can be trained in in situ simulations. The technical skills, at an early stage, can be trained in bench top models, pelvic trainers and with animal models. At an intermediate stage, more advanced skills can be trained on VR or transurethral resection of the prostate simulators [27]. Simulation and VR allow urologists to train situations which are extremely dangerous and cannot be practiced without putting a patient’s life at risk. Such simulations have been carried out in urology by training of an unexpected death scenario using realistic simulation of an operating room [28].
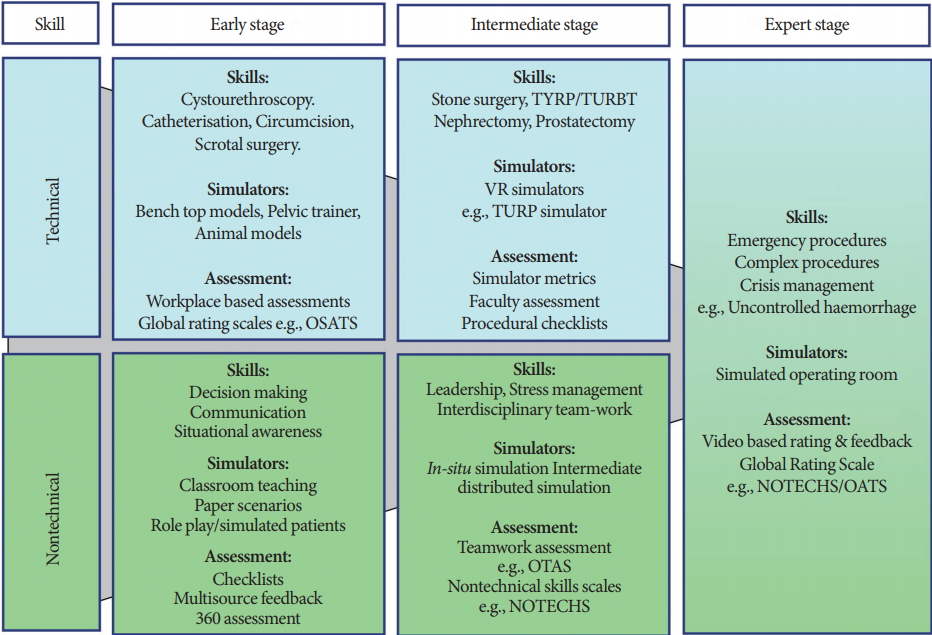
Framework for simulation across the urological training program. TURP/TURBT, transurethral resection of the prostate/ transurethral resection of bladder tumor; VR, virtual reality; OSATS, objective structured assessment of technical skills; OTAS, observational teamwork assessment for surgery; NOTECHS, nontechnical skills.
TECHNICAL SKILLS
Technical skills rank among the most important for surgeons and doctors. The predominant methods imply training with simulators. When learning minimalistic invasive surgery methods such as laparoscopy operation, surgeons need for example to learn to cope with the fulcrum effect [29]. This effect is a result of entering the body through small incisions and to force a rotation at the point where surgical instruments enter the body. Manipulating surgical instruments using these techniques requires intensive training. Especially in this case, the accuracy of haptic feedback is crucial, since forces and direction of movement are counter-intuitive [30]. The development of these psycho motor skills is essential.
The use of simulators in this field is uncontested. Table 2 shows a simplified version of the overview of the table mentioned by Brunckhorst et al. [24]. In addition to showing which simulation methods are available in VR or as bench top simulator, the research also analyzes the learning curves for various procedures. In this case it is the number of hours of training sessions necessary to become operational in a certain simulation. Eventually, the authors conclude with the recommendation for a curriculum as shown in Fig. 4 called a training pathway. Similar to the research by Arora et al. [27] shown in Fig. 3, both proposals include the idea of a module-based training program in urology education.
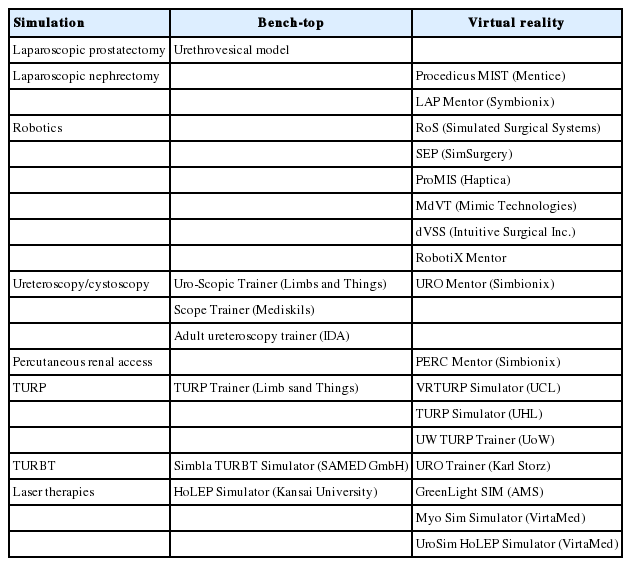
Overview simulations available for urology
Proposed training pathway for procedure-specific curricula.
Despite different approaches and premises, these 2 examples confirm the important position of simulation and AR/VR training in urology education. Modern urology workshops seem to rely particularly on simulation: A compact and innovative method of teaching multiple disciplines and skills to urology students is the earlier mentioned urology simulation boot camp [26]: for ten days the urology trainees follow dedicated lectures and training sessions, all of them accomplished using different simulation methods.
FUTURE IMPROVEMENTS WITH VIRTUAL REALITY AND SIMULATION
This section introduces 2 examples of recently emerging practices and attempts for new methods in bladder therapy and surgery. The examples are chosen because of their difference in order to demonstrate the broad possibility of applications. The first example shows the use of VR and simulation on the side of the patient as a potential new form of therapy. The second one demonstrates how VR and simulation are used to spread a new technology and provide the necessary training to a large number of urologists.
NEW THERAPY FOR TREATMENT OF PARURESIS
“Paruresis refers to the inability to initiate or sustain urination where individuals are present due to the fear of perceived scrutiny from others” [31]. Few therapies exist for this type of anxiety also called the “shy bladder syndrome” [32]. A study about a cognitive behavioral therapy example for Paruresis was published by Hambrook et al. [32]. While the overall result was subjectively perceived positive, many aspects remain to be researched. Exposure therapy could be a possible therapy for this behavioural disorder and the immersive features of VR could provide a solution for a new behavioral therapy. Lewis et al. [33] measured how VR can create the same stress inflicted to the patient by simulating the environment of a public toilet facility. While adapted exposed therapies need to be developed, the results indicate a potential for new applications and therapies using VR in this field.
TRAINING FOR TRANSURETHRAL RESECTION OF BLADDER TUMORS
New technologies and developments have improved and changed the practice and increased the success of cystoscopy with transurethral resection of bladder tumors (TURBTs) [34]. The new techniques increase accuracy in the diagnosis of cancer and new technologies in cystoscopy endoscopic management increase the safety and patient outcomes of bladder cancer. With the increased significance of developments in this field, it is important to adapt training methods in order to propagate their application. Virtual cystoscopy using VR seems to be predestined for this purpose. A recent study of Neumann et al. [35] showed that this training method can have multiple advantages: Short training methods can improve efficacy and safety of VR-TURBT. It can decrease the procedural time and it can reduce accidental bladder injury and blood loss [35]. Comparable to other box simulators enhanced with VR or AR methods this new training method could help to speed up the adoption of this new diagnostic and surgical practice.
CONCLUSION
While manufacturers predict a brilliant future and deploy numerous applications and businesses for AR/VR applications [36,37], reality shows that very few large software and hardware platforms exist. AR/VR remains a specialized niche market, as opposed to other modern education technologies such as Elearning, or classic text book learning [38]. Besides the small size of the market and the specialization for educational content, 2 particular factors may slow down the development: One capital concern in the entire field of education with AR/VR is the question of assessment: How are the performances of trainees evaluated? What is the feedback trainees obtain from a simulation?
The answer depends on the type of simulation: VR is ready for the training of nontechnical skills. This applies also to virtual labs as presented in a previous section. Despite their educational advantages and diverse applications, these technologies lack the accuracy and precision of haptic simulations. Together with the various E-learning platforms these teaching methods all use a more or less elaborate game scenario. The software compares the trainee’s inputs with a set of predefined correct answers.
Technical skills, however, are mostly trained with validated simulators. With those simulators, feedback and assessment can be a problem. Not all systems record and analyze the movements of a procedure. A solution can be a combination of dedicated simulation hardware enhanced with AR technology.
While looking at the best simulation techniques, it is important to mention that the experience and skills of urologists cannot merely be taught via simulation alone. A very crucial part is the feedback from an expert and the experience that can be gained through a fellowship. This is true for regular urology curricula as well as aforementioned workshops or boot camps. Simulation cannot replace this relationship or experience, but it can help to overcome obstacles such as time and distance and make the communication of a mentor and a urologist trainee easier and intensified. VR’s built-in communication capabilities can create new possibilities for telementoring, telemedicine, and telesurgery [39]. Technologically enhanced fellowships, can support the trainee by giving advice, expertise and feedback from an expert without the expert actually needing to be on location. These technologies could strengthen and facilitate human relationships and mentor procedures during the educational curriculum.
After examination of different application areas for VR and simulation and showing its potential in the field of bladder treatment and surgery, several conclusions regarding further development can be drawn:
Development of new therapies and new surgical methods also require new methods of training and practice. As technology and methods are constantly evolving, VR and simulation represent an efficient way of propagation for new technologies for the profession. They allow a large number of urologists to train and to practice methods intensively and safely before they can consider applying them to real patients.
The present article has shown 2 possible trends for the development of VR and simulation: As in the case of possible treatment of paruresis, simulation and VR could benefit the patient in an environment of reeducation and exposing behavioural therapies. Research shows that the simulation can create a similar type of stress stimulus like real environment situations. This is an important indicator and could open the field of VR and simulation to new kinds of therapy models in rehabilitation and exposure therapies.
The other case can be observed in the training of new methods for training diagnosis and surgery of bladder cancer. Following the trend of noninvasive surgery and evolving developments in endoscopy techniques, simulations and VR can help the urologists diagnose bladder cancer with more accuracy and perform the necessary TURBTs with more accuracy and higher safety for the patient.
Additional trends can be observed: VR and simulation applications are most likely to develop where education is dangerous and costly. Premium application will be simulations, where patients’ life might be in danger such as emergency situations. Also, the technology of VR offers the potential to complement human relationships in urological education. The new devices can enhance the possibilities of telementoring and allow sharing advice and experience even to remote areas.
The overall benefits of VR and simulation can be seen as strengthening competence and skills for the urologist trainees. As a result, an improvement in the quality of health care could be achieved by the sustained education of medical professionals.
Notes
Conflict of Interest
SJK, a member of the Editorial Board of INJ, is the third author of this article. However, she played no role whatsoever in the editorial evaluation of this article or the decision to publish it. No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
· Full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis: AH
· Study concept and design: AH
· Drafting of the manuscript: AH
· Critical revision of the manuscript for important intellectual content: SJK
· Administrative, technical, or material support: SJK
· Study supervision: SJK, TKW, KJC