The Prevalence of Lower Urinary Tract Symptoms and Overactive Bladder in South Korea: A Cross-Sectional, Population-Based Study
Article information

Abstract
Purpose
Lower urinary tract symptoms (LUTS) affect over half of the adults’ population worldwide, with an increasing prevalence among the older age groups. Therefore, with the increasing elderly population, LUTS is an important disease, highlighting the need for accurate data on its prevalence. This present study aimed to investigate the prevalence of LUTS in South Korea.
Methods
The study targeted individuals aged at least 19 years nationwide. We conducted computer-assisted telephone interviews, 80% mobile random digital dialing (RDD) sampling frame, and 20% landline RDD sampling frame between April and May 2020. Questionnaires included The International Prostate Symptom Score (IPSS), the overactive bladder symptom score (OABSS), and the characteristics of respondents. Current International Continence Society definitions were used for individual LUTS and OAB.
Results
There were 2,000 respondents, 1,009 (50.4%) were women and 546 (27.3%) were aged ≥60 years. Based on our IPSS questionnaire survey results, 77.9% of the respondents had LUTS; 63.7% had mild symptoms (1–7), 11.7% had moderate symptoms (8–19), and 2.4% had severe symptoms (20–35). The prevalence and severity of LUTS increased with age with 22.1% of respondents aged 60 years and above complaining of moderate or severe LUTS. According to the survey through OABSS, the prevalence of OAB was 9.6%, males were 10.3% and females were 9.0%.
Conclusions
Based on our survey results, 77.9% of the Korean adult population (over the age of 19) experienced at least one LUTS, and the severity increased with age. The prevalence and severity of OAB increased with age, especially after 40 years; the prevalence of OAB was 9.6%, and 13.4% of them were over 60 years old.
INTRODUCTION
Lower urinary tract symptoms (LUTS) include a variety of storage, voiding, and postmicturition symptoms. Overactive bladder (OAB) and stress incontinence are the main storage symptoms; voiding symptoms include slow or interrupted stream, terminal dribble, hesitancy, and straining; while incomplete emptying and postmicturition dribble are the key postmicturition symptoms.
OAB is a subset of storage LUTS defined as ‘urgency, with or without urgency incontinence, usually with frequency and nocturia’ [1,2]. LUTS especially storage symptoms (urinary incontinence and OAB), can have detrimental effects on the physical, psychological, social, and sexual well-being [3,4]. Previous studies have shown that LUTS affects over half of the adults’ population worldwide, with an increasing prevalence among the older age groups [5,6]. Therefore, with the increasing elderly population, LUTS is an important disease, highlighting the need for accurate data on its prevalence.
To achieve a high level of accuracy, the method of prevalence investigation is important. In particular, it must be an accurate representation of the demographic structure. In the present study, we investigated the prevalence of LUTS in Korea. In order to have an accurate representation of the demographic structure, the authors determined the survey targets and conducted a telephone survey, and calculated the number of samples by region and age.
MATERIALS AND METHODS
The present study targeted individuals aged at least 19 years nationwide. computer-assisted telephone interview (CATI), 80% of mobile random digital dialing (RDD) sampling frame and 20% of landline RDD sampling frame were conducted between April to May 2020. The questionnaire included the International Prostate Symptom Score (IPSS), OAB symptom score (OABSS), and characteristics of the respondents. The questionnaire included IPSS for assessing symptom bother, by which the severity was categorized into 4 groups: 0, no; 1–7, mild; 8–18, moderate; 19– 35, severe. The OABSS was used to define and classify OAB as mild, moderate, or severe. A score ≥2 for question 3 “How often do you leak urine because you cannot defer the sudden desire to urinate?” and an OABSS total score ≥3 were defined as having an OAB. OAB was divided into 3 groups according to the following scores: mild, a total score ≤5; moderate, a total score of 6–11; severe, a total score ≥12.
The population of South Korea in April 2020 was estimated to be 43,467,906 (Supplementary Table 1). In order to secure a stable sample size by city/province, a modified proportional allocation method (proportional allocation after priority allocation of 20 people) by sex and age was applied (Supplementary Table 2). Based on sex, age, and region (based on resident population released by the Ministry of the Interior and Safety at the end of April 2020), we calculated and applied weight as shown in Supplementary Fig. 1. The estimated sampling error of this study design was calculated 3.1%p as a 95% confidence interval. The overall fieldwork process proceeded as shown in Supplementary Fig. 2. Collected raw data were edited, coded, and cleaned before finalizing. Final data were analyzed by using IBM SPSS Statistics ver. 25.0 (IBM Co., Armonk, NY, USA).
The study was performed in compliance with Good Clinical Practice and in accordance with the Declaration of Helsinki. Since this study was based on CATI and RDD sampling methods, an Institutional Review Board approval was not considered necessary according to the Bioethics and Safety Act (Act No. 16372).
RESULTS
There were 2,000 respondents, 1,009 (50.4%) were women and 546 (27.3%) were aged ≥60 years. The characteristics of respondents according to the stratum are shown in Table 1. Results of the IPSS questionnaire survey showed that 77.9% had LUTS, among them, 63.7% had mild symptoms (1–7), 11.7% had moderate symptoms (8–19), and 2.4% had severe symptoms (20–35) (Fig. 1). Symptoms tended to increase and worsen with age; LUTS was present in 72.9% of the participants under the age of 60, and 89% of those over 60.
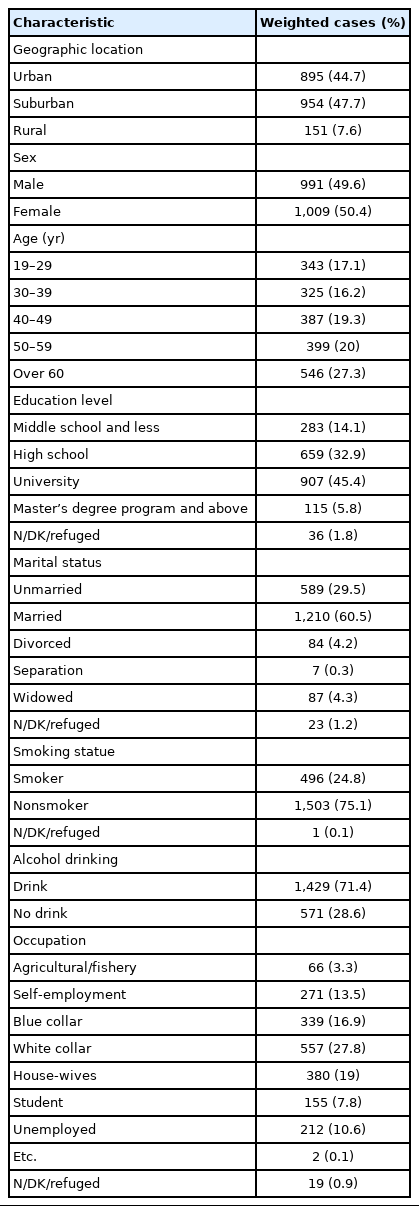
Characteristics of survey respondents (n=2,000)

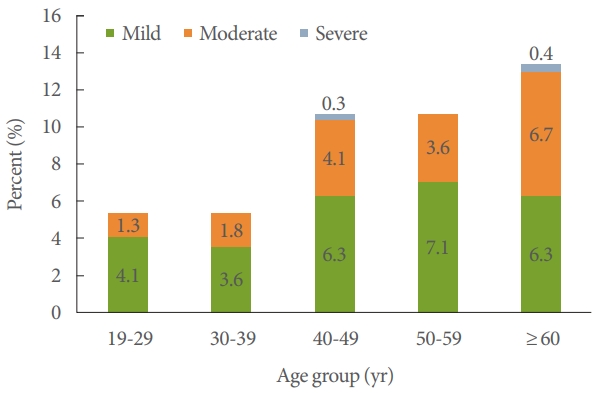
Prevalence of lower urinary tract symptoms according to the severity.
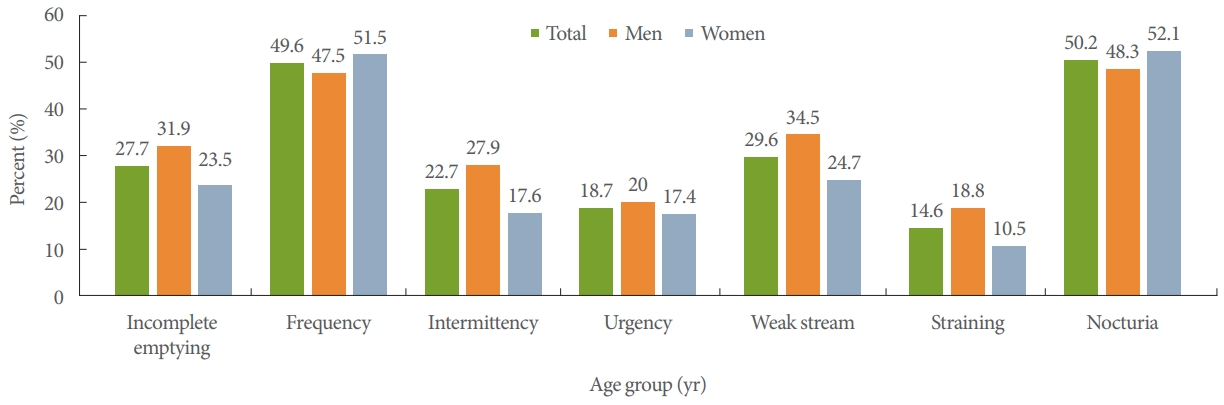
Of the reported LUTS, nocturia (50.2%) and frequency (49. 6%) were the most frequent, followed by weak stream (29.6%), incomplete emptying (27.7%), intermittency (22.7%), and straining (14.6%). Obstructive symptoms were more common in men while the prevalence of storage symptoms was the same in both men and women (Fig. 2).
Prevalence of lower urinary tract symptoms by sex.
The prevalence of OAB, as determined by the OABSS, was 9.6%, among the males were 10.3% and females were 9.0%. The prevalence of OAB in those under the age of 60 was 8% and 13.4% in those over the age of 60. The prevalence and severity of OAB increased with age, especially after 40 years (Fig. 3). The most prevalent symptom among the OAB symptoms was nocturia (men, 48.3%; women, 52.5%).
Prevalence of lower urinary tract symptoms by sex.
DISCUSSION
There are many LUTS prevalence surveys have been conducted worldwide, and although the survey methods applied and subjects were different, there are no significant differences in the prevalence reported; about half of the adults’ population have been reported to have LUTS, and the frequency increases with age. Expectedly, the major LUTS prevalence studies conducted in Korea do not show much difference from the international studies.
In a Korean EPIC study reported by Lee et al. [7] in 2011, the prevalence of LUTS and OAB were investigated by geographically stratified random samples from a population-based crosssectional telephone survey of men and women over 18 years of age. A total of 9,067 people were contacted and 2,000 people participated in the survey. The overall prevalence of LUTS was 61.4%, and the prevalence increased with age. Nocturia was the most common symptom, and the prevalence of OAB was 12.2%. Urinary incontinence was reported in 2.9% of the men and 28.4% of the women. In an internet-based survey of 2,080 men and women over 40 years of age, Yoo et al. [8] reported that the prevalence of LUTS was 68.2%, mild to moderate LUTS on IPSS were reported in 40.1% of the participants, and the prevalence of OAB based on OABSS was 19.7%. In a survey on the prevalence of LUTS conducted in China, Taiwan, and Korea, a total of 8,284 people aged 40 years and above participated in an internet-based self-administered survey, and the prevalence rate of LUTS was 62.8% for the men and 59.6 for the women [9].
Despite the consistency in the LUTS prevalence reported so far, the prevalence of OAB reported in Korea varies widely, from 5.2% to 29.9%. Kim et al. [10] analyzed the results of The Korean Community Health Survey in 2012 using OABSS. In this study, the prevalence of OAB in Korean adult women was 5.2%, and risk factors included age, body mass index, income and education level, marital status, and smoking.
Choo et al. [11] conducted a clinically validated computer-assisted telephone interview to investigate the prevalence of OAB in Koreans aged over 40 years. A total of 2,005 participants participated, and the prevalence was 20.8% for men and 31.3% for women.
In this study, the prevalence rate of OAB was 9.6%, males were 10.3%, and females were 9.0%. The prevalence of OAB increased significantly with age (P<0.001).
The inconsistencies in the prevalence could be attributed to the varying investigation methods. Several factors should be considered when developing an epidemiological study design. To achieve accuracy in epidemiologic studies, the selection of target populations, methods of sampling and investigation, and standardized questionnaires must be tailored to capture a sample that represents the general population [12]. Unfortunately, previously reported studies have investigated the prevalence of specific age groups in specific regions. However, this survey is a population-based study that extracted samples from all the regions across the nation and across a wide range of age groups in order to achieve a high level of accuracy. In addition, to further enhance accuracy, CATI were conducted using IPSS and OABSS.
Epidemiological investigations can be conducted through several survey methods including personal interview (PI), telephone interview (TI), postal survey (PS), and web survey. The choice of survey method can be influenced by several factors, such as cost, objectives, and target population. On the other hand, different survey techniques have varying mode effects that influence the participants’ response [13].
Conventionally, most epidemiologic studies on LUTS are conducted using PI or PS methods; the PS method is widely used since the 1960s owing to its lower cost, higher efficiency, and lower mode effects while the PS method is preferred because of its suitability for a large-scale survey. TI was first introduced in Western countries in the 1930s, but it was faced with population coverage challenges due to the low penetration rate of telephones at that time. However, with the increasing worldwide telephone penetration rate, the RDD technique, the TI method can achieve almost complete population coverage and therefore it is a potentially acceptable survey method. The TI method is less expensive, less time-consuming, and has a lower mode effect than the PI [14]. However, the development of technologies such as call block, caller identification, answering machines, and cellular phones has led to low response rates and reduced coverage of specific populations. Also, there are high chances of a social desirability bias with TI method, especially for sensitive questions such as urological problems [15]. CATI is an interview method used mainly in lifestyle and health care fields [16]. CATI has numerous advantages including a wide population coverage, minimized error incidences due to real-time recording of the responses, and simplified data handling. In comparison with the face-to-face interviews and PI method, CATI generally yields higher participation rates at a low cost [17].
In general, every survey method has its own strengths and weaknesses, therefore, a suitable method should be based on the specific conditions include the survey objectives, the target population characteristics, and affordability. Researchers can obtain information about well-acknowledged criteria for the specific clinical conditions of LUTS from existing epidemiologic studies [12].
In conclusion, this study is a population-based survey aimed at estimating the prevalence of LUTS and OAB in South Korea using the IPSS and OABSS questionnaire methods.
Based on our survey results, 77.9% of the Korean adult population (over the age of 19) experienced at least one lower urinary tract symptom, with severity increasing with age. The prevalence rate of OAB was 9.6%. Since the population structure changes as time changes, the prevalence of LUTS is also likely to change with time; therefore, we recommend periodic LUTS and OAB prevalence investigations.
SUPPLEMENTARY MATERIALS
Supplementary Tables 1 and 2 ands and Figs. 1 and 2 can be found via https://doi.org/10.5213/inj.2142112.056.
Supplementary Table 1.
Population status according to region, sex, and age
Supplementary Table 2.
Sample allocation stratified by age, sex, and region
Supplementary Fig. 1.
Weight calculation methods.
Supplementary Fig. 2.
Data processing.
Notes
Research Ethics
This research was supported by the Leading Foreign Research Institute Recruitment Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (MSIT) (NRF-2018K1A4A3A02060572).
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
·Conceptualization: MKK, JHL, WJC, DKK
·Data curation: MKK, JHL, WJC
·Formal analysis: MKK, WJC
·Funding acquisition: MKK
·Methodology: MKK, JHL, WJC, DKK
·Project administration: MKK
·Visualization: MKK, YSS
·Writing-original draft: MKK, YSS
·Writing-review & editing: MKK, YSS, JHL, WJC, DKK