Prevalence of Postprostatectomy Incontinence Requiring Anti-incontinence Surgery After Radical Prostatectomy for Prostate Cancer: A Retrospective Population-Based Analysis
Article information

Abstract
Purpose
This study aimed to examine the prevalence of surgery for postprostatectomy incontinence (PI) following minimally invasive surgery compared to conventional open surgery for prostate cancer.
Methods
This retrospective cohort study used the Florida State Ambulatory Surgery and State Inpatient Databases, 2008 to 2010, radical prostatectomy (RP) patients were identified using International Classification of Diseases (ICD)-9/10 procedure codes and among this cohort, PI was identified also using ICD-9/10 codes. Surgical approaches included minimally invasive (robotic or laparoscopic) versus open (retropubic or perineal) RP. The primary outcome was the overall prevalence of surgery for PI. The secondary outcome was the association of PI requiring anti-incontinence surgery with the surgical approach for RP.
Results
Among the 13,535 patients initially included in the study (mean age, 63.3 years), 6,932 (51.2%) underwent open RP and 6,603 (49.8%) underwent minimally invasive RP. The overall prevalence of surgical procedures for PI during the observation period among the all patients who had received RP was 3.3%. The rate of PI surgery for patients receiving minimally invasive surgery was higher than that for patients receiving open surgery (4.8% vs. 3.0%; risk difference, 1.8%; 95% confidence interval, 0.3%–3.4%). The adjusted prevalence of PI surgery for patients who had undergone laparoscopic RP was higher than that for those with retropubic RP (8.6% vs. 3.7%).
Conclusions
Among patients undergoing RP for prostate cancer, the prevalence of PI surgery is not negligible. Patients undergoing minimally invasive RP had higher adjusted rates for PI surgery compared to open approaches, which was attributed to high rate of PI surgery following laparoscopic approach and low rate of PI surgery following perineal approach. More studies are needed to establish strategies to reduce the rate of PI surgery after RP.
INTRODUCTION
Radical prostatectomy (RP) has been a standard treatment for localized prostate cancer (PCa) [1]. Although the oncological benefit of RP has been demonstrated in prospective randomized trials, particularly for men with intermediate and high-risk disease, patient quality of life (QoL) can be affected by postoperative complications that may include erectile dysfunction (ED) and postprostatectomy incontinence (PI) [2].
PI has been demonstrated to significantly reduce patient QoL [3], far outranking ED with respect to patient dissatisfaction following RP [4]. Although PI is of concern to surgeons and patients alike, investigations have reported varied prevalence of PI following RP. This is likely attributable to the accepted belief that PI will recover over time. Indeed, previous investigations have reported that 68% of patients regain complete continence by 2 months postoperation, with this number increasing to ~90% at 12- and 18-month postoperation [5,6]. However, several studies have indicated various rates of persistent PI ranging from 4%–30%, according to the definition of PI used [7]. Some studies have shown the prevalence of PI and their predictors by surgical modality, yet most of these studies were limited by small sample sizes, exclusion of young populations, lack of a detailed surgical approach, and short follow-up duration [5-7]. In view of the long-life expectancy associated with surgically treated PCa, maximizing patient QoL should be considered to be concurrent with PCa-specific survival [6,8]. Therefore, the true prevalence of long-standing, severely bothersome PI must be understood into order to select optimal treatment strategies for PCa.
The objective of this study is to examine the prevalence of PI requiring anti-incontinence surgery in patients receiving minimally invasive surgery and to compare this prevalence with conventional open surgery for PCa using large cohort data from the Healthcare Cost and Utilization Project National Inpatient Sample database.
MATERIALS AND METHODS
Data Source
A retrospective cohort study was performed using discharge data from Florida State Ambulatory Surgery and Services Databases and State Inpatient Databases, Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality (www.hcup-us.ahrq.gov/databases.jsp) to examine the prevalence of PI in patients receiving RP. These are all-capture state databases that contain patient characteristics, primary and secondary diagnoses, and procedures, and these databases afford the ability to link patients over time.
Patients
Patients receiving RP between January 2008 and December 2010 were identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 CM) procedural code. Patients with metastatic PCa were excluded from the study (ICD-9 CM codes 196, 197, 198, and 199). Due to missing variable information, a further 1,426 patients were excluded. All patients were followed up for at least 2 years after RP in order to track the prevalence of PI.
Main Exposures
Patients receiving open (60.5: retropubic or 60.62: perineal) or minimally invasive RP were identified using the ICD-9 procedural code. Using the ICD-9 procedural code or Current Procedural Terminology (CPT) code, minimally invasive surgeries were further differentiated to laparoscopic (ICD-9 CM: 54.21 or CPT: 55866) or robotic-assisted surgery (ICD-9 CM: 17.4x). The presence of PI was defined as the rate of PI surgery in this study and was identified by using affiliated ICD-9 CM procedure codes/CPT codes ensuring the anti-incontinence surgeries. Anti-incontinence therapies included 3 procedures: (1) sling operation; (2) artificial urinary sphincter (AUS) or inflatable device, and (3) bulking agent injection. Sling operation was identified using ICD-9 CM procedure codes (59.3, 59.4, 59.5, 59.6, and 59.7) and CPT codes (53440, 53443, 51840, and 51841). AUS or inflatable device was referenced using ICD-9 CM procedure codes (58.93) and CPT codes (53444, 53445, and 53449). Injection of the bulking agent was referenced using ICD-9 CM procedure codes of 59.72 and CPT code (51715).
Demographic and Clinical Characteristics
Hospital level data collected included location (urban or rural) and teaching status (teaching or nonteaching). Patient-related data included age, race (white, black, Hispanic, or other), household income (poorest, poor, wealth, wealthiest), and insurance status (private, Medicare, Medicaid, or other). The comorbidity condition of each patient was described using the Charlson Comorbidity Index. Household income was defined by medical household income by quantile distribution using zip codes. The annual hospital volume was estimated according to the number of procedures at a given patient’s hospital, and was defined as more than the 75% percentile (highest quartile).
Outcomes
The primary outcome was the overall prevalence of PI surgery. The presence of PI was defined as the rate of PI surgery in this study and was identified by using affiliated ICD-9 CM procedure codes/CPT codes ensuring the anti-incontinence surgeries. The secondary outcome was the association between prevalence of PI surgery with the surgical approach for RP (open vs. minimally invasive or retropubic vs. perineal vs. laparoscopic vs robot-assisted RP). The prevalence of PI surgery was defined as having either ICD-9 CM procedure code or CPT code along with or without any relevant ICD-9 CM diagnostic codes.
Statistical Analysis
Categorical variables were presented as numbers and percentages and were compared using chi-square tests. A weighted logistic regression model with inverse probability of treatment weighting (IPTW) was developed in order to adjust for potential confounders described in Table 1 at the baseline patient characteristics level. The weights used for patients undergoing open RP (retropubic or perineal) were the inverse of ‘1–propensity score’, and weights used for patients receiving minimally invasive RP (laparoscopic RP or robotic-assisted RP) were the inverse of just the propensity score, which were estimated by multiple logistic regression analysis without considering the outcomes. Log-binomial regression models were utilized in order to estimate risk ratios (RRs) for each procedure on PI. All models were adjusted for the clustering of patients within hospitals in order to adjust for interhospital variability. A sensitivity analysis was also conducted to determine whether the rate of PI surgery related to each surgical approach (open and minimally invasive) was influenced by the detailed surgical modality within each surgical approach (retropubic, perineal, laparoscopic, and robotic-assisted RP). During sensitivity analysis, a new IPTW was conducted in order to analyze the RR for each procedure, after adjustment for confounders. These analyses were not prespecified but rather conducted post hoc and should thus be interpreted as exploratory. Statistical analysis was performed using 2-sided tests with a significance level of <0.05 and Stata 14 (StataCorp LLC, College Station, TX, USA).

Baseline characteristics of patients receiving open and minimally invasive radical prostatectomy
RESULTS
A cohort of 13,535 patients undergoing elective minimally invasive (robotic-assisted RP: n=6,100 and laparoscopic RP: n=503) or open RP (retropubic: n=5,173 and perineal: n=1,759) has been included for final analysis. The demographic characteristics of this cohort are summarized in Table 1. Before the propensity weighting process, the open and minimally invasive RP cohorts differed in several variables, particularly age, insurance status, and annual hospital volume. Following propensity score weighting, similar covariate distributions were achieved between open and minimally invasive RP in the weighted populations (the standardized difference score was <0.2).
The overall prevalence of PI surgery during the observation period among those patients who had received RP between 2008 and 2010 was 3.3%. The crude rate of detailed anti-incontinence procedure was described in Table 2. The most common procedure for first treatment of PI was the sling procedure (1.8%), followed by injection of a bulking agent (0.8%), and AUS in 0.6% of cases.
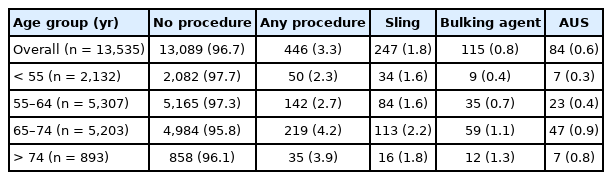
Crude frequency rate of anti-incontinence procedure by age group
The unadjusted prevalence of PI surgery was similar between the open and minimally invasive groups (Table 3). However, the IPTW-adjusted prevalence of PI surgery for patients receiving minimally invasive surgery was higher than for those who received open surgery (4.8% vs. 3.0%; RR, 1.60; 95% confidence interval [CI], 1.16–2.20).

Unadjusted and adjusted absolute risk differences and risk ratios for postprostatectomy incontinence in patients undergoing minimally invasive and open radical prostatectomy, 2008–2010
For each of the 4 surgical modalities, the unadjusted prevalence of PI surgery is presented in Table 4. The IPTW-adjusted prevalence of PI surgery for patients receiving perineal RP was lower than that for those with retropubic RP (0.6% vs. 4.3%; RR, 0.13; 95% CI, 0.07–0.23). However, the IPTW-adjusted prevalence of PI surgery for patients receiving laparoscopic RP was higher than for those with retropubic RP (8.6% vs. 3.7%; RR, 2.36; 95% CI, 1.20–4.64). The unadjusted and IPTW-adjusted prevalence of PI surgery was similar between retropubic and robotic-assisted RP.

Unadjusted and adjusted absolute risk differences and risk ratios for postprostatectomy incontinence in patients undergoing robot-assisted, laparoscopic, perineal, and retropubic radical prostatectomy, 2008–2010
DISCUSSION
To the best of our knowledge, this study is the first to define the prevalence of PI surgery following RP in a large cohort analysis, while simultaneously investigating for differences in the prevalence of PI surgery according to the initial surgical modality employed, including retropubic, perineal, laparoscopic, and robotic-assisted RP. The main outcome of our study was to present the overall prevalence of PI surgery in this large cohort sample and to compare the difference of risk of PI surgery according to the type of surgical modality used. The prevalence of PI surgery reported in this study (3.3%) was lower than those that have been previously reported in the literature (4%–6%), which might have resulted from the differences in the definition of PI used, the follow-up period, and the inclusion of study population [7,9-11]. Moreover, this study revealed that the rate of PI surgery for patients undergoing the minimally invasive RP was higher than patients receiving open surgery in the adjusted analysis, which was mainly due to the high PI prevalence of laparoscopic RP.
Out study has several strengths, including the utilization of a population-based dataset and comparison of RP surgical approach. Considering the time-dependent clinical manifestation of PI after RP, it is reasonable to use the objective definition of the need for an anti-incontinence procedure as a representation of the most bothersome or severe urinary incontinence. Two previous large observational studies have shown similar prevalence rates of PI necessitating intervention using the similar definition as that used by our study. Kim et al. [12] reported that the prevalence of PI was 6%, according to Surveillance, Epidemiology, and End Results (SEER) cancer registry data linked with Medicare claims from 2000 to 2007. Similarly, Lowrance et al. [13] reported the prevalence of PI to be 5.45% using SEER cancer registry data linked with Medicare claims from 2003 to 2005.
Older age is strongly associated with the prevalence of PI, and previous large studies using Medicare data have been limited to patients 65 years older, whereas our study is more inclusive of younger ages [12,13]. Further, these studies of older patients have demonstrated slightly increasing PI rates with prolonged follow-up, which is likely attributable to other factors that influence incontinence (overactive bladder, sarcopenia) as men get older [11,14]. Therefore, our study provides critical information for patients under 65 years of age requiring RP surgery since it includes a substantially longer follow-up period than previous studies. Only 2 studies have shown a follow-up duration similar to our study, with a median of 20 months and a minimal duration of 24 months [12,15].
To date, there has been controversy over whether minimally invasive procedures including robotic-assisted or laparoscopic RP are equivalent in terms of risk of PI compared to open RP. Due to the lack of randomized, controlled investigations comparing RP surgical procedures, it is difficult to conclude which surgical type (s) is superior. Several studies confirm that open RP and robotic-assisted RP have equivalent outcomes oncological outcomes [16]. Recently, Sujenthiran et al. [15], using a large administrative database, reported that robotic-assisted RP showed significantly better functional outcomes postoperatively, including nonspecific urinary and stricture-related complications, compared to open and laparoscopic RP. However, the definition of urinary complications used in this study included intervention codes that were not specific to PI, but included all types of urologic procedures of the urethra, prostate, and bladder. Other studies have shown that robotic-assisted RP shows lower rates of perioperative complications (blood transfusions, shorter time of catheter use postoperatively, shorter length of hospital stay), postoperative complications (PI and ED), and positive surgical margin rates compared to open approaches [17,18]. O’Neil et al. [19] reported that, relative to open RP, patients undergoing robotic-assisted RP had higher rates of early recovery of sexual function and continence. However, Barry et al. [17] reported that robotic-assisted RP was not associated with better outcomes compared to PI in their retrospective cohort analyses. Moreover, Hu et al. [20] reported that the use of minimally invasive procedures including either robotic-assisted or laparoscopic RP increased 5-fold from 9.2% at 2003 to 43.2% at 2006–2007, with patients receiving minimally invasive procedures reporting increased genitourinary complications (4.7% vs. 2.1%) and a greater likelihood of a PI diagnosis (15.9 vs. 12.2 per 100 person-years, P=0.02).
When comparing the prevalence of PI procedures between laparoscopic and open RP, our data also support previous reports suggesting that laparoscopic RP yields the highest prevalence of necessitating PI procedures. Huang et al. [21] reported lower rates of PI and ED for robotic-assisted RP compared with laparoscopic RP in a recent meta-analysis. Lowrance et al. [13] reported that PI necessitating anti-incontinence intervention in 5.0% of open RP cases and 6.2% of laparoscopic RPs, respectively.
One unique feature of our study population is that it includes a substantial number of men who underwent perineal RP. Perineal RP yielded the lowest prevalence of PI surgery significantly lower relative to the other 3 RP modalities. Our results support the studies by Bishoff et al. [22] and Harris [23] which both reported that perineal RP is associated with the lowest rates of PI and was more cost-effective compared with retropubic RP. The lower rates of PI surgery we observed in perineal RP might explain the recent finding that use of a posterior approach is associated with better continence and potency rates compared to conventional anterior approaches [24].
Our study does have several limitations. First, as this data originates from one geographical area (Florida), the results might be influenced by local practice patterns that limit generalization to other populations. Second, limited information exists regarding clinically-relevant variables including disease characteristics, surgeon volume, and factors influencing patient choice of therapy, surgical approach, and surgeon that could influence their outcomes with regard to PI, as well as their later choice to have a procedure for PI. Third, although we demonstrated risk difference and RR, additional analyses investigating the possible causative factors of PI requiring surgery were not possible. Possible reasons for higher rates of PI surgery in the minimally invasive RP group include a greater expectation regarding clinical outcomes for robotic-assisted RP relative to open RP, a steeper learning curve for robotic-assisted RP, and the emergence of new robotic-assisted RP surgical techniques [25]. Fourth, conversion rates from minimally invasive to open RP were not captured, although previously reported rates are low [26]. Fifth, the actual prevalence rate of severe and bothersome PI is under captured through procedural codes because of coding errors and since some men might not elect for surgery despite having severe symptoms. Sixth, this study could not consider surgical factors including postoperative membranous urethral length. Recently, Cho et al. [27] highlighted the importance of saving the membranous urethral length as long as possible in terms of continence recovery. Finally, long-term data are necessary in order to compare longer functional outcomes, especially those related to QoL, between open and minimally invasive procedures
In conclusion, among patients undergoing RP for PCa, the prevalence of PI surgery is not negligible. Patients undergoing minimally invasive RP had higher adjusted rates for PI surgery compared to open approaches, which was attributed to high rate of PI surgery following laparoscopic approach and low rate of PI surgery following perineal approach. More studies are needed to establish strategies to reduce the rate of PI surgery after RP.
Notes
Fund/Grant Support
This work has been supported by Soonchunhyang University Research Fund.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
·Conceptualization: IGJ, THB, JB, BC
·Data curation: JHK, YK, THB
·Formal analysis: JHK, YK, BC
·Funding acquisition: JHK
·Project administration: IGJ, BC
·Writing-original draft: JHK, IGJ
·Writing-review & editing: JHK, YK, THB, JB, BC