‚ÄĘ HIGHLIGHTS
- Saphenous nerve stimulation have different effects on bladder reflex depending on stimulus frequency.
- Also, it may be a potential therapeutic mechanism of tibial nerve stimulation.
INTRODUCTION
Sacral neuromodulation or sacral nerve stimulation is the U.S. Food and Drug Administration-approved therapy that treats 2 opposite bladder conditions: overactive bladder (OAB) and nonobstructive urinary retention, which is a characteristic of the underactive bladder (UAB) [1-3]. However, this technique has not been applied widely because it is 2-staged invasive and complicated implantation process. Also, many patients cannot afford the high cost of the procedure. Hence, increasing attention has been focused on exploring the effects of minimally invasive peripheral nerve electrical stimulation on the bladder function.
Tibial nerve stimulation (TNS) is a third-line treatment option for OAB patients who are refractory to conservative therapies [4]. The stimulation amplitude is equal to or below the intensity threshold (T) inducing foot motor [5]. However, animal studies indicated that required intensities causing bladder inhibition are greater than those used clinically [6,7]. This disparity is currently under investigation. Anatomical studies showed that the posterior branch separated from the main trunk of the saphenous nerve passes through the approximate location where the needle electrode of percutaneous TNS (PTNS) or the surface electrode of transcutaneous TNS (TTNS) is placed [8,9]. The animal studies in rats and clinical investigation confirmed that saphenous nerve stimulation (SNS) at 20-Hz frequency inhibits the bladder reflex and be used for treating OAB [10-12]. Therefore, some researchers speculated that the saphenous nerve is coactivated, and there may be a potential action mechanism during TNS therapy [13]. Thus, animal experiments are needed to test this hypothesis.
Interestingly, a recent animal study in cats showed that SNS at 1-Hz frequency induced bladder excitation and restored the bladder capacity (BC) to normal level [14]. The present study provided a novel neuromodulation therapy for UAB that is valuable when the reflex of the bladder with a large capacity is underactive. Based on the above studies, it seems that the effects of SNS on the bladder function depend on the frequency of stimulation. Previous studies demonstrated that pudendal nerve stimulation (PNS) at 3‚Äď15 Hz inhibits the bladder, while stimulation at 20‚Äď50 Hz evokes bladder contractions [15,16]. Similarly, TNS at low frequency (2 Hz) and high frequency (5‚Äď20 Hz) evokes excitatory and inhibitory bladder responses, respectively [17]. Our recent study also showed that sacral dorsal root ganglion (DRG) electrical stimulation at low frequencies (3‚Äď7 Hz) inhibited isovolumetric rhythmic bladder contractions, while excitatory effects were observed at 2 frequency ranges: low frequencies (0.25‚Äď1.5 Hz) and middle frequencies (15‚Äď30 Hz) [18]. Irrespective of SNS at 1-Hz frequency under normal bladder reflex activity, excitatory bladder effects have yet to be investigated.
The goals of the current study were as follows: (1) to determine the effects of different SNS stimulation frequencies on bladder reflex with normal saline infusion; (2) to evaluate the effects of combined SNS and TNS stimulation on bladder activity to explore a putative TNS therapeutic mechanism.
MATERIALS AND METHODS
Surgical Procedure
The experiments were conducted in 13 randomly selected adult cats (9 males and 4 females, 6‚Äď12 months old, weighing 2.3‚Äď3.1 kg). The animal care and use committee at Capital Medical University approved all protocols involving the use of animals in this study (AEEI-2020-141). Each animal was anesthetized with isoflurane (2%‚Äď5% in oxygen) during surgery and switched to intravenous őĪ-chloralose (65 mg/kg, supplemented as needed) during data acquisition. The anesthetic and fluid were administered via the left cephalic vein. The heart rate and blood oxygen level were monitored throughout the experiment. The body temperature was maintained by a heating pad. A middle abdominal incision was made to expose the bladder, and the ureters were separated (the left was ligated, and the right was externally drained). A 2-lumen catheter was introduced into the bladder via a small cut on the proximal urethra and secured by a ligature around the urethra. One lumen of the catheter was used to infuse the bladder with normal saline at the rate of 1-2 mL/min after connecting to a pump. The other lumen was connected to a pressure transducer (MP150; BIOPAC Systems, Inc., Camino Goleta, CA, USA) to measure the bladder pressure.
The left saphenous nerve was exposed via an incision along the medial aspect slightly above the knee joint. Another incision was made on the medial side of the contralateral hindlimb above the ankle to expose the tibial nerve for stimulation to avoid the ipsilateral muscle excessive fatigue. Two custom-fabricated bipolar nerve cuff electrodes (platinum contacts) were implanted on the 2 nerves, and electrical pulses were given out by an external stimulus generator (Master-8; AMPI, Jerusalem, Israel). Subsequently, the incisions were closed after the surgery.
Stimulation Protocol
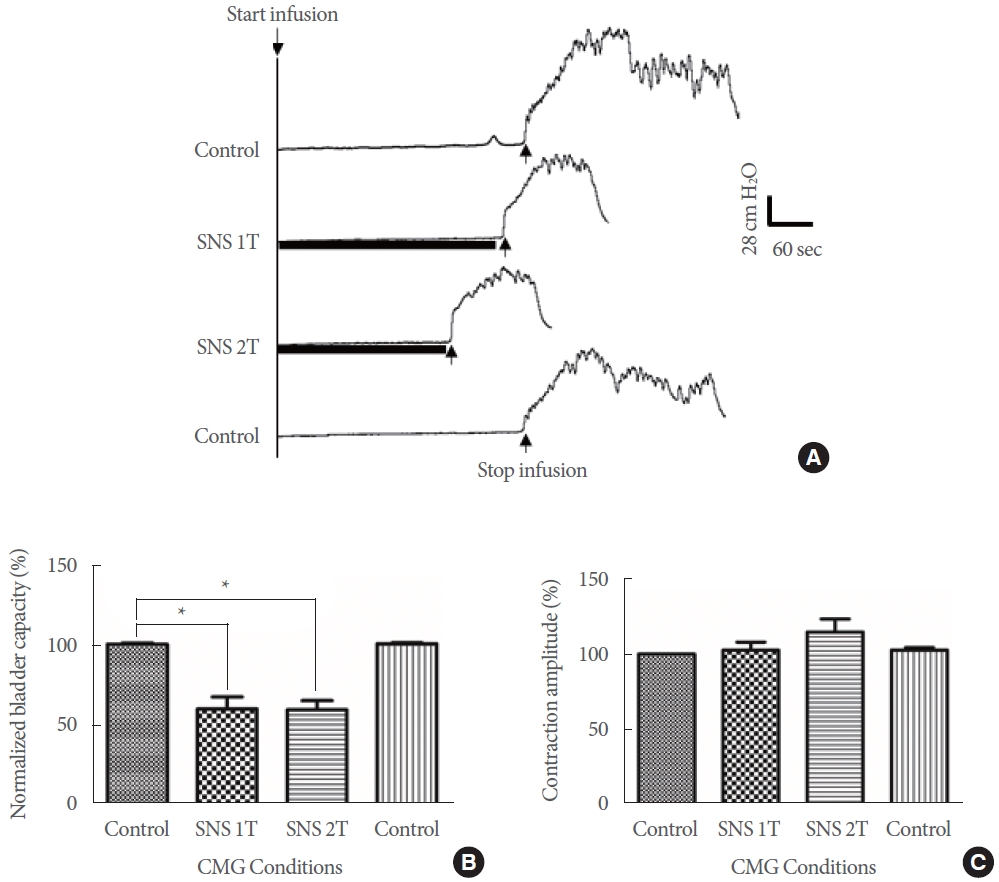
Approximately 30 minutes after surgery, a series of acute experiments were started. BC was used to test the inhibitory or excitatory effects of the stimulation. The bladder was drained before each experiment. After the appearance of the first large amplitude (>30 cm H2O) and long duration (>20 seconds) bladder contraction, the bladder infusion was stopped [14]. BC was defined as the volume of infusion into the bladder. Initially, after emptying the bladder, 2 or 3 cystometrograms (CMGs) were obtained without stimulation that served as the control BC.
After the BC stabilized, stimulation was applied during sequential CMGs. Uniphasic rectangular pulses (0.2-msec pulse width) were delivered to the 2 nerves. The threshold, T, was defined as the minimal intensity for inducing observable muscle twitches on the posterior thigh, hip, or toe for the saphenous nerve and toe twitches for the tibial nerve. First, the frequencydependent effects of SNS at 3 different frequencies (1, 5, and 20 Hz) were tested in a randomized order. Second, 6 CMGs were performed to evaluate the effects of combined SNS and TNS stimulation: (1) control CMG without stimulation; (2) CMG with TNS (20 Hz, 1T); (3) CMG with SNS (20 Hz, 1T); (4) CMG with TNS (20 Hz, 2T); (5) CMG with combined SNS and TNS stimulation (20 Hz, 1T); (6) control CMG again to determine any poststimulation effect. The bladder was emptied after each CMG, pausing for a 3-4-minutes rest between successive CMGs to allow the bladder to recover.
Statistical Analysis
Prism ver. 8.0 (GraphPad Software, La Jolla, CA, USA) was used for statistical analysis. To compare the sequential CMG recordings, the BCs were normalized to the measurement of the first control CMG, and calculated as follows: normalized BCs= Cs/BC of the first control CMG√ó100%. The amplitude of maximal bladder contractions was also measured. Repeated measurements under the same conditions in the same animal were averaged. All summary data are expressed as the mean ¬Ī standard error. One-way analysis of variance, followed by Bonferroni multiple comparisons, was used to determine the statistical significance (P<0.05).
RESULTS
Frequency-Dependent Effects of SNS on Bladder Reflex
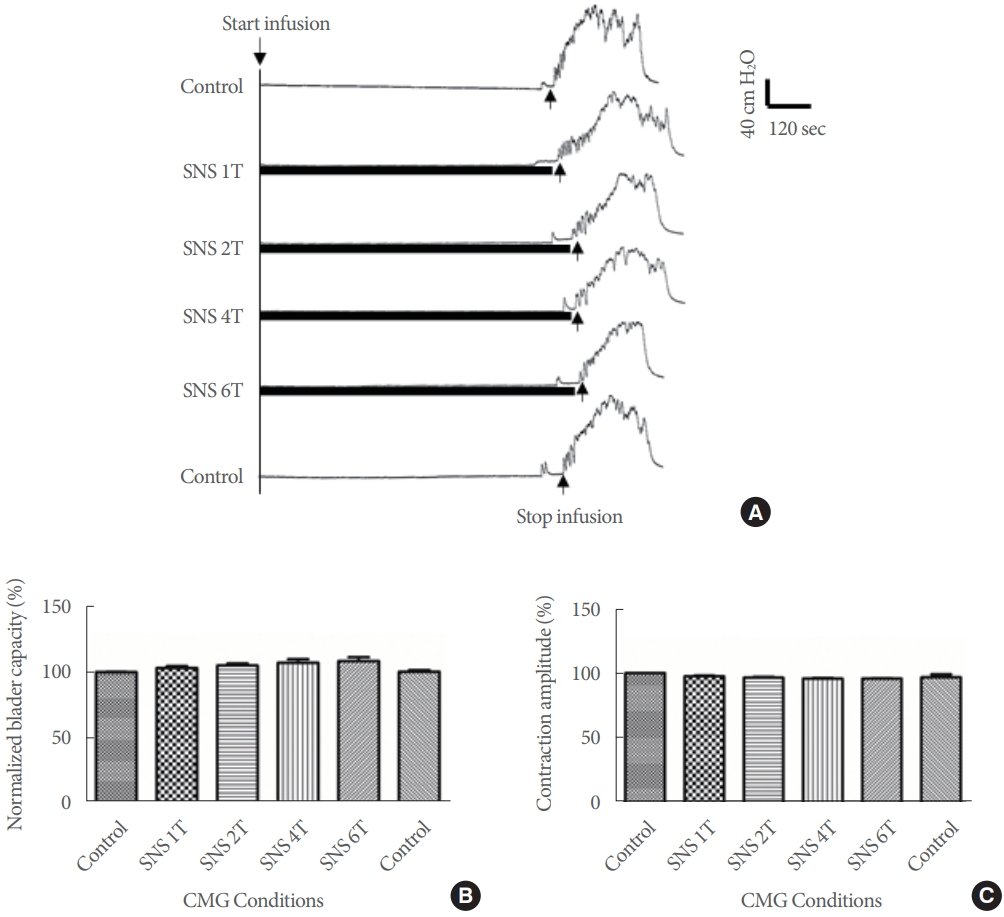
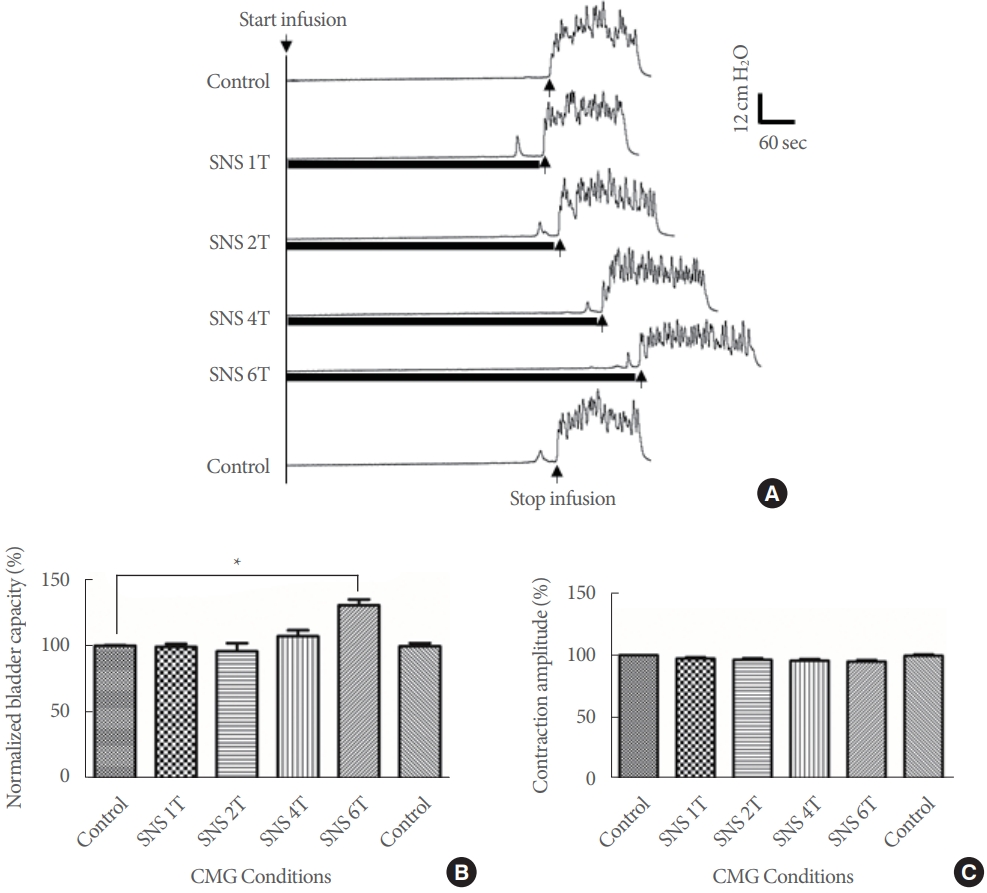
SNS at 1 Hz significantly reduced BC to 59.8% ¬Ī7.7% and 59.3% ¬Ī5.8% of the control level at 1T and 2T, respectively (P<0.05). However, no significant difference was detected between the 2 intensities (P>0.05) (Fig. 1). When examined at 5-Hz frequency, no significant effects on the BC were detected in the results obtained using 1‚Äď6T intensities (P>0.05) (Fig. 2). SNS (20 Hz) at intensities of 1‚Äď4T did not significantly change the BCs (P >0.05), while it was significantly increased to 130.6% ¬Ī4.2% of the control level at 6T (P <0.05) (Fig. 3). Moreover, the BCs returned to the prestimulation levels without any poststimulation effects at the 3 frequencies and SNS at 1‚Äď15 Hz did not significantly change the maximal contraction amplitude of micturitions (Figs. 1‚Äď3).
Combined Bladder Inhibition of Simultaneous SNS and TNS
TNS and SNS at 20 HZ did not significantly change the BCs at 1T, respectively (P >0.05), while TNS at 2T significantly increased the BC to 128.3%¬Ī3.8% of the control level (P<0.05) (Fig. 4). When SNS was combined with TNS at 1T, it significantly increased the BC to 122.7%¬Ī1.9% of the control level and induced an inhibitory effect similar to that TNS at 2T (Fig. 4). The combined stimulation also significantly increased the BC compared to separated TNS and SNS at 1T (P<0.05) (Fig. 4). There were no significantly change about the maximal contraction amplitude of micturitions during different nerve stimulation (Fig. 4).
DISCUSSION
The results of the current study revealed a frequency-dependent role of SNS as it could not only decrease the BC at 1 Hz but also inhibit the bladder activity and increase the BC at 20 Hz (Figs. 1, 3). Previous studies suggested that the stimulating frequency is a critical parameter that mediates the modulatory effect on bladder activity. A study of electrical stimulation of pudendal nerve trunk in cats showed that PNS at 3 Hz inhibited the reflex bladder activity and significantly increased the BC, while that at 20 Hz induced large bladder contractions [15]. Another 2 studies about selective stimulation of pudendal nerve branches in the cat also reported the frequency-dependent characteristics: inhibited detrusor activity of dorsal genital nerve (5‚Äď10 Hz) and sustained bladder contractions of cranial sensory (‚ȧ5 Hz), dorsal genital (‚Č•20 Hz), and rectal perineal (‚ȧ10 Hz) [16,19]. Moazzam et al. [17] performed an acute study in anesthetized cats and concluded that TNS at low frequency (2 Hz) and high frequency (5‚Äď20 Hz) could evoke excitatory and inhibitory bladder responses, respectively. Our recent study in cats also showed that TNS (0.5‚Äď3 Hz) induced large amplitude and sustained bladder contractions when the bladder was underactive, while in OABs, TNS inhibited the bladder overactivity at 5 Hz [20]. Another our recent study in cats explored the excitatory and inhibitory effects of stimulation of sacral DRG on bladder reflex in cats [18]. Herein, we found that stimulation at low frequencies (3‚Äď7 Hz on S1 or S2 DRG) significantly inhibited isovolumetric bladder contractions, while excitatory effects were observed at 2 frequency ranges: low frequencies (0.25‚Äď1.5 Hz on S1 DRG and 0.25‚Äď1.25 Hz on S2 DRG) and middle frequencies (15‚Äď30 Hz on S1 and S2 DRGs). But we did not investigate the effects of contraction amplitude and time during the voiding phase and whether SNS at 1 Hz had an excitatory effect or not must be explored in the future study.
Compared to the TNS, there are only a few studies about SNS. The study by MacDiarmid et al. [10] presented the initial experience in treating OAB patients by SNS. Electrical stimulation was applied at a frequency of 20 Hz for 30 minutes and repeated weekly for 12 weeks. Positive response to SNS was achieved in 14 of 16 patients (87.5%), and no obvious adverse events were reported. Two studies investigated the acute effects of SNS in rats at different frequencies (2, 5, 10, 20, and 50 Hz) [11,12]. The studies indicated that SNS at 20 Hz evoked bladder inhibitory effects and was effective in increasing the BC, which was in agreement with the current results. Other frequencies resulted in nonsignificant effects. Our results showed that SNS at 20 Hz inhibited bladder activity, while that at 5 Hz did not have any effect on the bladder activity even if applied at a high intensity (6T) (Figs. 2, 3). However, TNS at both 5 Hz and 20 Hz could inhibit the bladder activity at lower intensity (2T‚Äď4T) as compared to SNS (20 Hz, 6T), indicating a difference between the 2 types of peripheral nerve neuromodulations. Due to the superficial location of the saphenous nerve, SNS may also be achieved with a chronically implanted device or by a transcutaneous modality similar to TNS used in clinical practice [21,22]. The inhibited effects of SNS need to be validated in further prospective, randomized, controlled studies. A recent study establishing the animal model of UAB in cats showed that SNS at 1-Hz frequency induced bladder excitation and restored the BC to normal level when the bladder reflex is underactive with a large BC [14]. The current study investigated the effects of SNS at 1 Hz frequency under normal bladder reflex activity (Fig. 1). It could significantly reduce the BC as compared to the control level. Our recent study also established an animal model of UAB in cats by PNS [23]. Additional studies are essential to verify whether SNS at 1 Hz under a PNS-induced underactive state is effective. Interestingly, a similarity was noted between TNS and SNS as both could evoke excitatory effect at a low-frequency stimulation (TNS at 2Hz and SNS at 1 Hz) [14,20].
In clinical practice, TNS is recommended as a third-line therapy for treating OAB [24]. The stimulation intensity is confirmed by the appearance of toe fanning or sensations radiated along the foot. However, most patients have been reported to experience painful sensations at the motor T [25]. Hence, it is set at one level equal to or below the intensity T [5]. On the contrary, significant inhibitory effects are evoked at 2T‚Äď4T in anesthetized cats and 3T‚Äď6T in anesthetized rats [6,7,17,26]. The saphenous trunk separates into major branches, which innervate the anterior and posterior regions of the lower leg in humans [8]. The posterior branch appears to overlap the region where the stimulation electrodes are applied during PTNS/ TTNS therapy [8,9,12]. In addition, the preclinical and clinical studies demonstrated that SNS at 20-Hz frequency inhibits the bladder reflex and is used for treating OAB [10-12]. Therefore, it is hypothesized that the saphenous nerve is coactivated during TNS treatment and is a potential therapeutic mechanism of TNS therapy [10-13]. However, to the best of our knowledge, the coactivated mechanism has not yet been investigated in animal experiments. The current results proved for the first time that SNS was involved in the process of TNS. TNS or SNS at 1T alone did not inhibit the bladder reflex. However, the combined stimulation at low intensity (1T) significantly increased the BC and suppressed the bladder activity, which did not differ significantly from the stimulation effects by TNS at 2T (Fig. 4). Our initial results indicated that (1) SNS played a role in the inhibition of the bladder activity during TNS, rendering it to be a potential underlying therapeutic mechanism; (2) SNS in combination with TNS maximized the clinical efficacy at a low intensity that could be a novel treatment modality for OAB. Single SNS at 20 Hz inhibited the bladder activity at a high intensity (6T); however, only a low intensity (1T) was required during the combined stimulation. Notably, the small stimulus effect induced by SNS is indeed the ‚Äúbarrier‚ÄĚ that TNS must pass through from 1T to 2T.
Nevertheless, the present study has some limitations. First, we only investigated the acute effects of SNS and combined neurostimulation in the current study, while TNS and SNS are delivered chronically in patient stimulation [10,25]. Thus, the effects of long-term therapy warrant further studies. Second, we established a study for the novel neuromodulation and provided the initial results of SNS at 3 different frequencies. A range of different frequencies from low to high remains to be explored in future studies. It is also necessary to determine the stimulation frequency that is safe for long-term usage. Third, bladder reflex contractions in the current study were evoked by normal saline infusion, which primarily activated the nonnociceptive bladder afferent fibers under physiological conditions. However, under pathological conditions, bladder irritation by acetic acid infusion activates nociceptive afferent fibers [27]. Although similar results were observed in the studies involving cats infused with saline and acetic acid [28], additional studies are imperative to confirm the effects of SNS in OAB cats. In the last, we stopped the nerve stimulation immediately before bladder contraction and did not investigate the effects of SNS during the voiding phase. whether SNS at 1 Hz had an excitatory effect or not must be explored in the future study.
In summary, the current study indicated that SNS reduced and increased BC depending on different stimulation frequencies. The combination of SNS and TNS maximized the clinical efficacy at a low intensity, and SNS may be a potential therapeutic mechanism of TNS. Therefore, additional preclinical and clinical studies would provide an in-depth insight into the benefits of SNS at different stimulation frequencies on long-term therapy in patients.