INTRODUCTION
Over 50% men aged ≥60 years develop lower urinary tract symptoms (LUTS) [1,2]. Benign prostatic hyperplasia (BPH) is one of the most common benign conditions associated with reduced quality of life [3,4]. It may present as conditions such as LUTS, acute urinary retention (AUR), urinary tract infections, and hematuria [5]. BPH increases the risk of mortality and morbidity, and the cost of BPH treatment is high.
The etiology of BPH is unclear, and the known risk factors include old age and hormones including androgen and estrogen [6]. Multiple factors are associated with this benign condition in old age. Jeong et al. [7] have reported that patients with severe LUTS are at increased risk of depression, especially nocturia, which is a risk factor associated with depression. In our previous study, the severity of BPH increased with age, and the treatment pattern in BPH patients varied according to the socioeconomic status [8]. Several other factors, such as physical activity, body mass index, stress level, and smoking history have been associated with the severity of LUTS [9].
The treatment for BPH is diverse, ranging from drug therapy to a combination of both drug therapy and surgical treatment. However, there are limited studies on the prevalence and treatment pattern of BPH. Further, an optimal treatment plan is necessary in some patients to achieve the best clinical outcome. Therefore, we conducted a cross-sectional study on the prevalence and treatment pattern, including the types of drugs used and surgeries performed, of BPH using nationwide data.
MATERIALS AND METHODS
Study Cohort
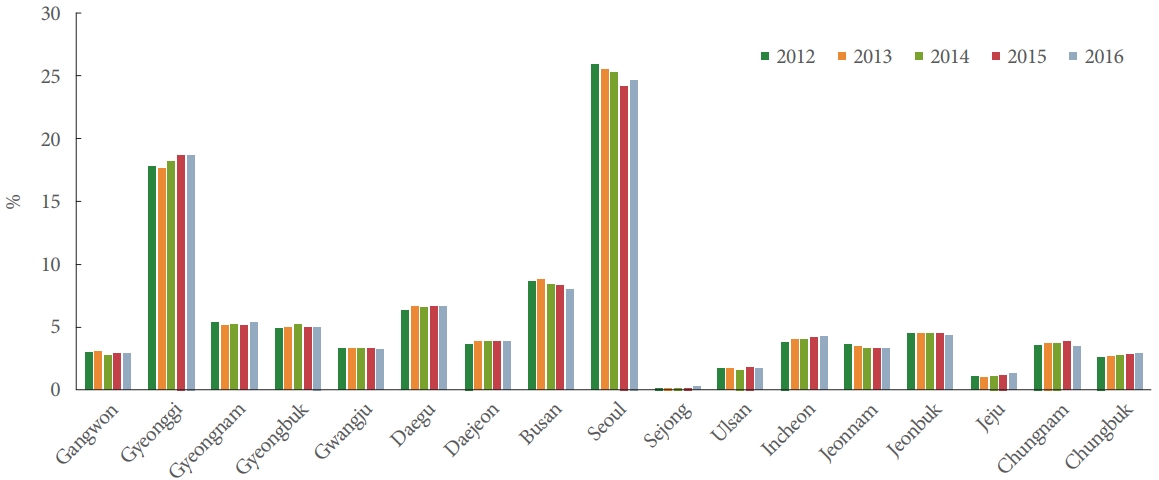
We performed a cross-sectional study about BPH treatment procedures using nationwide data sample after approval from the Institutional Review Board of Hanyang University Hospital (HY-2020-07-022). We obtained information on BPH treatment trends from the Health Insurance Review and Assessment Service-Aged Patient Sample (HIRA-APS). We used data on men aged ≥60 years from 2012 to 2016 from the database. We divided the cohort into 3 groups according to age —60–69 years, 70–79 years, and ≥80 years. Our study analyzed the regional distribution of BPH population according to the year.
Patient group setting (selected according to the following criteria)
(1) Patients with BPH code N40 more than once within a year
(2) Patients who underwent urology treatment
(3) Age ≥60 years (excluded condition: <60 years)
Code N40: Hyperplasia of prostate without complication (N400); Adenofibromatous hypertrophy of prostate without complication (N400.01); Enlargement (benign) of prostate hyperplasia (N400.02); Hypertrophy (benign) of prostate without complication (N400.03); Median bar (prostate) of prostate without complication (N400.04); and Prostatic obstruction of prostate NOS without complication (N400.05)
Primary Outcome
We classified the type of institution and other variables using HIRA-APS codes.
The treatment pattern of BPH was evaluated according to the type of institution. The institutions were classified as primary clinics (hospitals, including clinics) and secondary and tertiary centers. We analyzed the medication and operative trends of BPH. The medication trends were categorized as the 5-α-reductase inhibitor (5-ARI); 5-ARI and α-blocker; 5-ARI, α-blocker, and anticholinergics; and anticholinergics and α-blocker groups.
The operative trends were categorized as the holmium laser enucleation of the prostate (HoLEP), transurethral resection of the prostate (TURP), GreenLight laser, and prostatectomy groups.
The data were analyzed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) as mentioned above.
RESULTS
Treatment Trends of BPH
The number of BPH patients who were treated at clinics and tertiary centers showed an increasing trend every year. This pattern was observed for all treatment methods, including surgery and combination treatment. Treatment with medications was the most commonly used treatment option in >90% cases. As the number of patients increased, the medication usage trend also increased. Moreover, both surgery and combination treatment showed an increasing pattern.
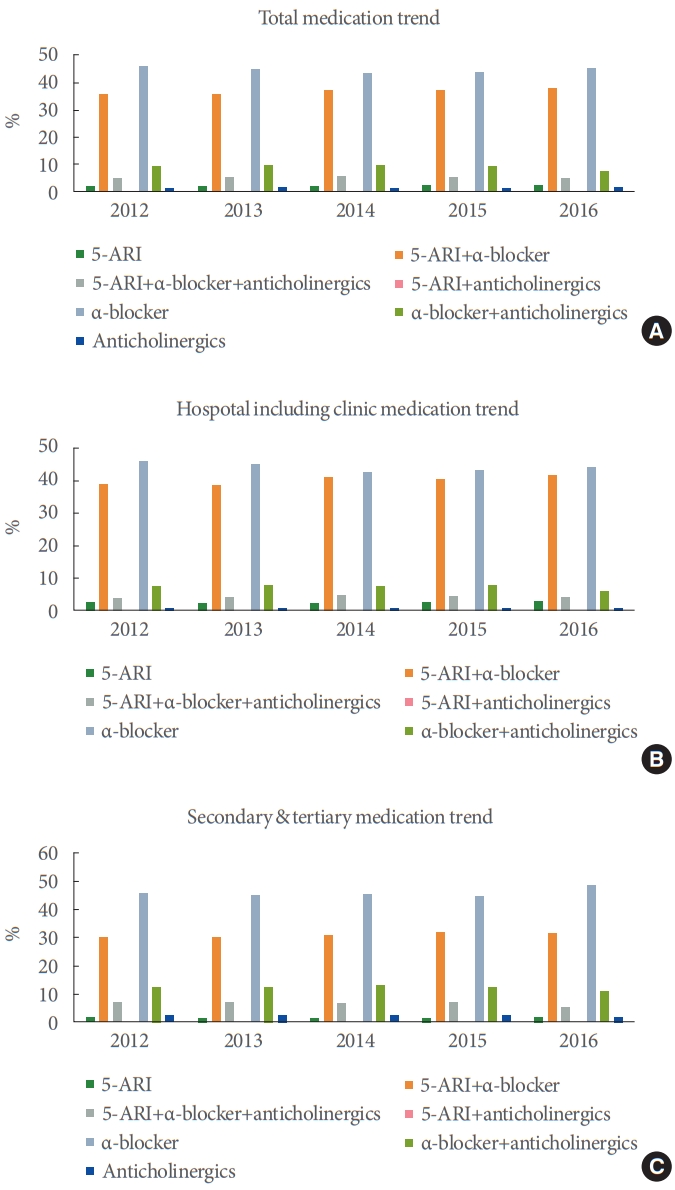
Medication Treatment Trend
Alpha-blockers were the most common medication recommended for BPH treatment, followed by a combination therapy of α-blocker and 5-ARI. A similar pattern (combination pattern such as α-blocker and 5-ARI) was observed in both clinics and tertiary centers throughout the study period (Fig. 2). Anticholinergics also used a combination therapy, but it was not ordinary use monotherapy. Medication trends of α-blockers and combination therapies are shown in Fig. 3.
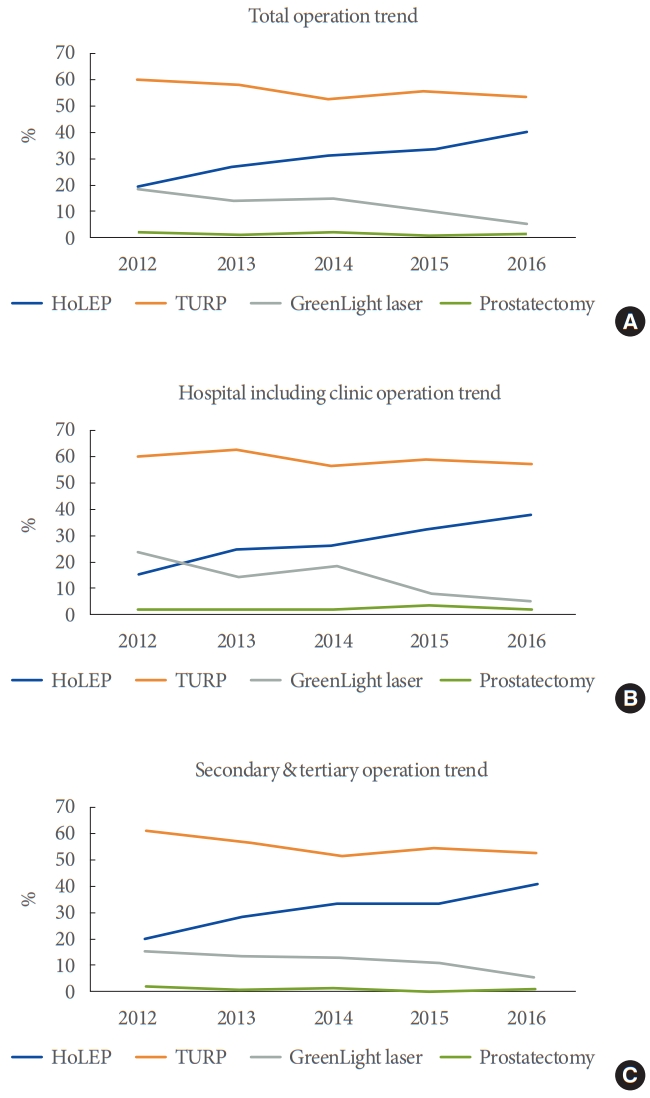
Surgical Treatment Trend
TURP was the most common surgical method for BPH treatment (60.2% in 2012; 57.9% in 2013; 54.7% in 2014; 56.0% in 2015; and 53.1% in 2016) (Fig. 4). However, TURP and greenlight laser treatments showed a decreasing pattern, while HoLEP showed an increasing pattern over the study period (20.5% in 2012; 25.6% in 2013; 29.5% in 2014; 33.5% in 2015; and 40.2% in 2016). This pattern was similar in both clinics and tertiary centers during the study period.
DISCUSSION
We analyzed the treatment pattern of BPH in South Korea using nationwide data. The number of BPH cases showed an accelerated increase in the superaged society. Although drug therapy was the common choice of treatment, surgical treatments showed an increasing pattern in our study. HoLEP showed an increasing pattern with the spread of the holmium laser use in South Korea.
Souverein et al. [10] analyzed the trend of BPH medications use from the PHARMO Record Linkage System. Their data showed that there was an increase in its use from 1.9/1,000 in 1,991 to 25.1/1,000 in 2,000. They also analyzed the trend of surgical procedures for BPH treatment and reported a cumulative incidence of 15.2%. Among the 5,671 men analyzed, TURP was the most common BPH-related prostatic surgery performed (13.4%). Our cohort also showed TURP to be the most common surgical treatment; however, HoLEP showed an increasing trend every year.
Due to the risk associated with surgical procedures for BPH, the use of α-blockers increased compared to that of 5-ARIs (hazards ratio, 1.52; 95% confidence interval [CI], 1.24–1.87). Malaeb et al. [11] analyzed the surgery trends for BPH from 2000 to 2008 using data from the Medicare carrier file. The surgical treatment pattern of BPH showed a reducing trend from 126,067 in 2005 to 101,195 in 2008. A diametrical relationship was observed between the medication and surgical treatment pattens of BPH in various countries. In the analysis of patients who only received medications for BPH treatment, the use of α-blockers only (78%, n=518) was the most common, followed by use of 5-ARIs only (9%, n=52) and a combination of both medications (13%, n=53) [11]. In our study, a similar pattern was observed with pharmacotherapy used most popularly for BPH treatment, and the use of α-blockers only was the most common medication trend.
Izard et al. [12] reported a declining pattern of surgical treatment for BPH from 1988 to 1998 in Canada.
Vela-Navarrete et al. [13] analyzed the medical records of patients undergoing surgical treatment for BPH from 1992 to 2002 in Spain and reported a decrease of over 17.6% in the number of surgical treatments performed in BPH cases. Moreover, pharmacotherapy showed an increasing trend from 46% in 1992 to 82% in 2002 (P<0.01) for BPH treatment, and the most common drug therapy used was α-blockers only (79%). Cindolo et al. [14] analyzed data from administrative and medical databases in Italy. They analyzed data on approximately 100,000 men aged >40 years over a period of 5 years. In this report, the medication trend for BPH increased by 43%. Moreover, almost 25% increase in the use of combination medication was observed in men aged >75 years. The contribution of 5-ARIs was greater in combination therapy than α-blockers (49% vs. 41%).
Since the introduction of 5-ARIs, the treatment trend has been changed to reinforce pharmacotherapy as the first treatment option [15].
In South Korea, Choi et al. [16] analyzed the BPH treatment patterns between 1985 and 2009. They categorized the 3 analysis periods as group 1 (1985–1989), group 2 (1995–1999), and group 3 (2005–2009). The comorbidities in their cohort increased over time, and this finding was different from that of a previous study. Elkoushy et al. [17] reported the variety in the characteristics of patients who underwent surgical treatment with laser for BPH. They categorized patients based on when the surgery was performed as follows: before April 2004, between April 2004 and March 2009, and from April 2009 to August 2014. They found that patients who underwent surgical treatment were older and had more comorbidities than those who underwent pharmacotherapy.
However, other studies showed different trends [18,19]. Borth et al. [19] evaluated the BPH treatment trends in patients during different periods.
Mayer et al. [18] analyzed the data from randomized clinical trials on surgical treatment performed for BPH between 1997 and 2007. They analyzed 3,470 patients from 67 studies on characteristics and surgical outcomes of BPH patients, and there was no significant difference in age over time.
He et al. [20] reported that AUR negatively affected the outcomes in patients undergoing surgical treatment for BPH. Among the patients undergoing bipolar TURP, those with preoperative AUR showed longer duration of hospitalization (≥90 hospital days) than those without preoperative AUR (10.7±0.9 days vs. 6.4±0.9 days, P<0.001). Reich et al. [21] found that preoperative AUR also affected the risk of postoperative voiding failure (12.0% vs. 3.5%; odds ratio, 3.78; 95% CI, 3.20–4.45). Djavan et al. [22] suggested that the high-risk group of treatment failure could be defined by chronic urinary retention (CUR) >1,500 m or age ≥80 years in men. Negro et al. [23] showed that the high-pressure CUR group showed poor clinical outcomes with respect to the International Prostate Symptom Score and postvoid residue (PVR).
As mentioned previously, delayed treatment could lead to increased risk of treatment failure. A previous study suggested that specific patient groups were at a high risk of progression when they were treated using only long-term medications without surgical treatment [24].
We found that pharmacotherapy only was the most common treatment trend for BPH. In this situation, some patients may show negative effects due to long-term pharmacological treatment. Long-term pharmacological treatment may mask asymptomatic progressive detrusor impairment, leading to gradual rise in PVR [25].
Blatt et al. [26] evaluated the relationship between detrusor variables, such as muscle cell size, muscle cell shape, and collagenosis, and the risk of postoperative voiding failure. Previous reports have suggested strategizing optimal treatments in patients with high risk of progression and using only medication treatment [27]. It is unclear in which patient group would surgical treatment be the optimal treatment.
With better insight into the key factors causing urinary complications, urologists can determine the most appropriate treatment method or follow-up depending on individual risks or progress [28]. In our study, TURP was the most common surgical treatment, but HoLEP showed an increasing pattern as the surgical treatment for BPH. Our results reviewed the treatment pattern of BPH and showed that pharmacotherapy was the most common treatment for BPH, especially only α-blocker therapy.
Our study has some limitations. First, it is a potential bias to reflect actual non-BPH such as urinary stone cases. However, it is not major portion of BPH code, BPH code without α-blocker is larger than BPH code with α-blocker. And it is not all of urinary stone patients with BPH code with α-blocker. Second, our data set did not cover 50s years old patients with BPH. There are many patients with BPH in 50s years old. We’ve chosen HIRA-APS due to major portion of BPH deviating older men.
In conclusion, the prevalence of BPH in men aged >60 years in South Korea showed an increasing trend in from 2012 to 2016. The major treatment method for BPH was drug therapy, and the use of α-blockers only was the most popular treatment pattern observed in Korea. Although TRUP was the most popular surgical method used for BPH previously, its trend showed a relative reduction during the studied period, whereas HoLEP showed an increasing pattern as the surgical treatment for BPH in South Korea. Thus, the surgical treatment pattern of BPH has changed from TURP to HoLEP.