Is There a Correlation Between Behçet Disease and Lower Urinary Tract Symptoms?
Article information

Abstract
Purpose
In this study, we aimed to determine the prevalence of lower urinary tract symptoms (LUTS) in patients with Behçet disease (BD) and to investigate the relationship between the severity of BD and LUTS.
Methods
Fifty-five patients with BD were included in this study from January to December 2018. All patients received a detailed urological evaluation. Additionally, BD activity was investigated using the Behçet Disease Current Activation Form. The International Prostate Symptom Score (IPSS), International Consultation on Incontinence Questionnaire Short Form, 8-item overactive bladder questionnaire forms, uroflowmetry, and postvoid residual urine volume were evaluated.
Results
The mean age of the patients was 42.6 years. The mean activity score of BD was 4.6±3.2 and the mean IPSS score was 7.3±7.3. Sex had no significant effect on the BD activity score. The BD activity score was significantly correlated with the IPSS score, frequency of daytime urination, nocturia, and urgency. It was also correlated with the presence and the severity of urinary incontinence and the effect of urinary incontinence on daily life. Peak flow rate, voided volume, and the postvoid residual urine volume were not correlated with the BD activity score.
Conclusions
LUTS were highly prevalent in patients with BD, and the severity and current activity of BD were correlated with frequency, nocturia, urgency, and urinary incontinence. Therefore, a urological evaluation of patients with BD in whom the activity and severity of the disease is elevated should be carried out comprehensively and patients should be managed accordingly.
INTRODUCTION
Behçet disease (BD), which was described by the Turkish dermatologist Hulusi Behçet and is characterized by the symptom triad of oral aphthous ulcers, genital ulcers, and uveitis, is a chronic systemic inflammatory disease of unknown etiology that affects the mucosa, skin, eyes, gastrointestinal tract, joints, blood vessels, and neurological system [1,2]. BD is endemic in the Middle East and in the Mediterranean region, as well as along the Silk Road, extending into Central and East Asia. It is also seen all over the world due to migration events [3,4]. BD can be seen at any age and in both sexes. While BD has a female predominance in countries such as USA, Korea, Spain, Brazil, and Sweden, it is more frequent in males in countries such as Turkey, Germany, Iran, and Greece [5]. The disease begins in the second decade of life, regardless of race or sex [6,7]. Its prevalence was reported to be between 20.8 and 35.7 per 100.000 in different countries [5].
BD affects all physiological systems since it is a multisystemic disease, although oral aphthous ulcers are the most common symptom [1,4,8]. Genital ulcers, ocular lesions, skin lesions, and gastrointestinal, cardiac, vascular, neurological, and pulmonary system involvement can also be seen. Involvement of the urogenital system manifests as urological problems such as epididymitis and sterile urethritis, in addition to genital ulcers [9]. In the literature, studies on the lower urinary tract (LUT) involvement of BD are rare. In a recent review published by Alizadeh et al. [10], the most common symptoms involving the LUT were reported to be storage symptoms and incontinence. However, urinary symptoms and urinary retention may also occur. In this study, we aimed to determine the prevalence of lower urinary tract symptoms (LUTS) in patients with BD and to investigate the relationship between the severity of BD and LUTS.
MATERIALS AND METHODS
Inclusion and Exclusion Criteria
Ethical approval for this study was granted by the local human subjects research ethics committee. Patients aged between 18 and 60 years who received care at the rheumatology and dermatology departments of 2 university hospitals between January and December 2018, and were diagnosed with BD according to the international BD working group criteria, were included in this study. Patients who had benign prostate hyperplasia, urethral strictures, urinary tract cancer, urinary tract infection, pelvic organ prolapse, a history of urinary incontinence surgery, pregnancy, and neurological diseases were excluded. Patients with a history of taking any medication that could affect the lower urinary system (alpha-blockers, anticholinergics, β3-adrenergic agonists) were also excluded.
Study Protocol
Finally, 55 patients who met the inclusion criteria and provided informed consent were included in the study. All patients received a detailed urological evaluation. Additionally, BD activity status was investigated using the Behçet Disease Current Activation Form (BDCAF), which was created by Bhakta in 1994 (with a minimum score of 0 and a maximum score of 12). At the urology outpatient clinic, the International Prostate Symptom Score (IPSS), the International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF), the 8-item overactive bladder questionnaire (OAB-V8) forms, uroflowmetry, and postvoid residual urine volume were evaluated. Demographic and clinical data were recorded.
Maximum flow rate (Qmax), mean flow rate, and voided volume were measured by uroflowmetry (MMS, Laborie Medical Technologies, ULC, Mississauga, ON, Canada) with the patient having sensation and sufficient desire to void, and postvoid residual urine volume was measured by transabdominal ultrasonography.
Statistical Analysis
The tests to be used in the comparisons for statistical evaluation were decided according to the central limit theorem. Data were analyzed in IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA) using descriptive statistics (number, percentage, mean, standard deviation) and statistical analysis tests (the Mann-Whitney U-test and the Pearson correlation test). P-values <0.05 were considered to indicate statistical significance.
RESULTS
The mean age of the patients (27 men and 28 women) was 42.6 years (range, 20–59 years). The mean ages of the male and female participants were 43.1±9.4 and 42.1±9.6 years, respectively. The mean instantaneous activity score of BD was 4.6±3.2 (3.8±2.8 for men and 5.5±3.3 for women). The baseline demographics of the patients and the manifestations of BD are presented in Table 1.

Baseline demographics of the patients and Behçet disease (BD) manifestations
The mean IPSS score (0–30) was 7.3±7.3 (7.0±7.0 for men and 7.7±7.6 for women). According to the IPSS scores, 60% of the patients had mild LUTS, 14.5% had moderate symptoms, and 15.5% had severe symptoms. According to uroflowmetry tests, the mean Qmax was 13.4±8.5 mL/sec (11.3± 7.0 mL/sec for men and 15.5±9.6 mL/sec for women). The mean voided volume was 315.1 ±189.1 mL (315.5 ±178.7 mL in men and 314.8±202.8 mL in women) and the mean postvoid residual urine volume was 22.4 mL (18.9 mL for men and 26.1 mL for women). Details about the patients’ LUTS are shown in Table 2.

The prevalence and the frequency of lower urinary tract symptoms in the patients
We found no significant effect of sex on the BD instantaneous activity score (P=0.057). Table 3 shows correlations between the duration and current activity score of BD and LUTS. The correlation analysis showed that the BDCAS was significantly correlated with the IPSS score, frequency of daytime urination, nocturia, and urgency. It was also correlated with the presence and the severity of urinary incontinence and the effects of urinary incontinence on daily life. Peak flow rate, voided volume, and postvoid residual urine volume were not significantly related with the BDCAS. The duration of BD was only correlated with patients’ age, not with any of the LUTS.
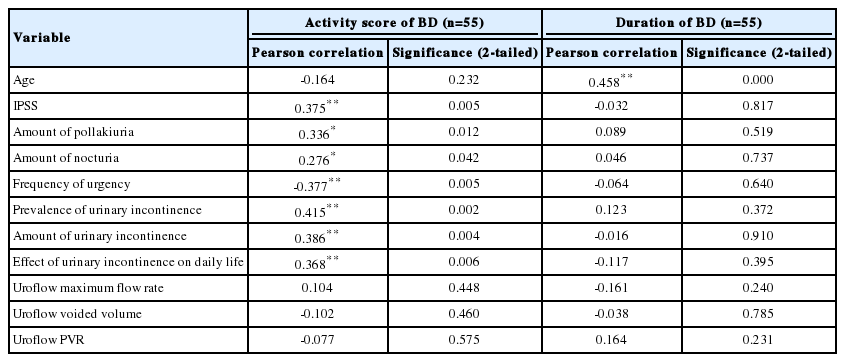
The correlation between the duration and current activity score of Behçet disease (BD) and lower urinary tract symptoms
None of the male patients’ medical history revealed any findings suggestive of epididymitis and none of them had received any previous treatment for LUTS.
DISCUSSION
According to studies on the LUTS of BD, genitourinary system involvement mainly consists of genital ulcers, epididymitis, urethritis, and cystitis [9,11]. Epididymitis has been evaluated in terms of urologic involvement in some studies investigating the activity index related to BD [12-14]. Although BD affects the urogenital system, and such problems are seen frequently, research investigating the LUT involvement of BD is limited. In this study, we demonstrated that LUTS were highly prevalent in patients with BD and that the severity and current activity of BD was correlated with those symptoms, such as frequency, nocturia, urgency, and urinary incontinence.
LUT involvement in BD disease was previously investigated with a primary focus on bladder involvement in a few case reports and case series with limited number of patients, most of whom were young to middle-aged men, and the most common symptoms were storage symptoms and, rarely, urge incontinence [10]. However, the majority of these studies were epidemiological in nature and to our knowledge, LUTS were not previously compared according to the severity or the current activity of BD.
Cetinel et al. [15] reported that the prevalence of bladder involvement in BD was 0.07%. However, that report only included patients who had severe bladder involvement, of whom 38% had augmentation cystoplasty. Another study from the same center including 104 male patients showed that the frequency of LUTS was between 5.8% (impaired force of urine) and 30.8% (nocturia) and that storage symptoms were more prevalent than voiding symptoms in patients with BD [16]. In our study, we found that the most prevalent LUTS were urinary incontinence (69.1%) and that 20% of patients had nocturia. Similarly, Erdoğru et al. [17] reported that BD patients had more incontinence and irritative bladder symptoms. Most previous studies found lower rates; however, in those studies, LUTS were evaluated by questions asked during interviews, and validated forms such as the IPSS, ICIQ-SF, and OAB-V8 were not used widely.
In patients with BD, self-healing ulcers or mass lesions that may resemble bladder tumors have been reported during cystoscopic examinations of the bladder [10,15,16]. These lesions are usually due to vasculitis [10]. In the study of Cetinel et al. [16], 2 of 8 patients had bladder ulcers and indurated, hypervascular lesions on cystoscopy. However, as indicated above, that study included only patients with severe symptoms. In the other study by the same group that included 104 male patients, the frequency of LUTS was higher in patients with BD, but cystoscopic examinations were not performed in any of the patients. Urodynamic evaluations in patients with BD revealed that the most common urodynamic finding was detrusor overactivity [15]. We did not perform cystoscopy or urodynamic tests in any of our patients because the aim of our study was to evaluate the correlation of LUTS with BD activity using symptom scores and questionnaires, and these tests would be unnecessarily invasive.
Regarding the voiding symptoms, 60% of the patients in our study had mild LUTS, 14.5% had moderate symptoms, and 15.5% had severe symptoms, according to the IPSS scores. In the study of Cetinel et al. [16], 62.6% of patients with BD had no obstructive symptoms and 29.8% of the patients had mild and 7.6% had moderate obstructive symptoms using a modified version of the Boyarsky symptom score. Uroflowmetry showed that the mean Qmax was 13.4±8.5 mL/sec (11.3±7.0 mL/sec for men and 15.5±9.6 mL/sec for women). The mean Qmax in male patients in our study is lower than has been reported in similar cohorts in the literature [18]. Karandreas et al. [19] reported that the Qmax and postvoid residual urine volume were normal in BD patients, while bladder sensation was increased.
Ocular, neurologic, and vascular involvement are recognized as the major causes of morbidity and mortality in patients with BD. Male patients are more often and more severely affected by these organ manifestations [20]. Neurologic involvement (neuro-BD), which has been reported in 5% to 10% of patients with BD, may also involve the brain stem [10,21]. Therefore, the involvement of the pontine micturition center was suggested as a reason for LUTS in BD. In the study of Cetinel et al. [15] 5 of 8 patients (62.5%) had neurological involvement. We excluded patients with any neurological symptoms from our study, but found that LUTS were still highly prevalent, suggesting that these symptoms might be due to direct bladder wall involvement and vascular involvement instead of, or in addition to, neuro-BD.
Although many activity index evaluation forms have been developed for BD, the BDCAF, which was developed by Bhakta in 1994, is the most commonly used [22]. Subsequently, the validity of BDCAF has been tested in several clinical studies [22-25]. We calculated the activity score using the validated Turkish-language form of this questionnaire in our study. The IPSS, ICIQ-SF, and OAB-V8 forms were used to evaluate the relationship between the activity score and LUT findings, instead of asking separate questions about urological symptoms, as in previous research.
Our study is not without limitations. Although BD is rare and the number of recruited patients was limited, as in previous studies, further studies with a larger number of patients would enable further analysis. Another limitation of our study might be the lack of a control group. Although we designed this study to determine the prevalence of LUTS and to investigate the correlations of these symptoms with the current activity of BD, a control group would make it possible to compare these findings with the normal population. However, our previous population-based prevalence study on LUTS can be used as a reference for the same population to overcome this issue [26].
In conclusion, although previous studies have suggested that bladder involvement and LUTS in patients with BD are due to neurological involvement, we demonstrated that when patients with any neurological symptoms were excluded, LUTS were still highly prevalent, suggesting direct bladder wall involvement and vascular involvement instead of, or in addition to, neuro-BD. The severity and current activity of BD were found to be correlated with LUTS such as frequency, nocturia, urgency, and urinary incontinence. Therefore, urological evaluations of patients with BD in whom the activity and the severity of the disease is elevated should be carried out comprehensively, and proper treatment options should be offered.
Notes
Research Ethics
Ethical approval for this study was granted by the local human subjects research ethics committee (Pamukkale University noninvasive clinical research ethics committee approval number: 60116787-020/36964)
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
·Conceptualization: AB, AEZ, OA, ZAY
·Investigation: AB, AO, SC
·Formal analysis: AB, YO, OA
·Methodology: YO, SC
·Project administration: AEZ
·Writing - original draft: AB, AEZ, ZA
·Writing - review & editing: AB, ZA