INTRODUCTION
Pediatric overactive bladder (OAB), which involves spontaneous or provoked detrusor contractions, can be detected during urodynamic testing if the childŌĆÖs bladder is full, in accordance with the specifications of the International ChildrenŌĆÖs Continence Society; this condition may cause frequency, urinary urgency, incontinence, and nocturia, with major impacts on daily life [1-3]. A recent study reported that OAB occurs in 15%ŌĆō20% of children, with a higher prevalence in boys; however, its prevalence declines with age, from 23.0% at age 5 to 12.2% at age 13 [4,5].
Currently, our understanding of the etiology and pathophysiology of OAB is incomplete, which is reflected by the lack of adequate treatment. Studies have found that in 42% to 70% of children with OAB, standard urinotherapy with a timer watch is effective [6,7]. However, 2%ŌĆō4% of children discontinue medication because of its low efficacy and associated side effects [8]. Transcutaneous electrical neural stimulation (TENS) is a nonpharmacological, noninvasive modality that has been clinically used as an alternative treatment for children with OAB [9]. Its advantagesŌĆöincluding its noninvasive and painless nature, as well as a lack of adverse reactions and drug interactionsŌĆöare expected to make TENS a more predominant choice of treatment modality. However, due to limitations in the the quantity and quality of previously published analyses, there is still insufficient evidence to demonstrate the efficacy of TENS by a pooled analysis of randomized controlled trials (RCTs).
Therefore, we performed this meta-analysis to evaluate the effect of TENS treatment in children on urodynamic indexes and objective OAB symptoms.
MATERIALS AND METHODS
Protocol
The Preferred Reporting Items for Systematic Reviews and Meta-analysis guideline was followed in this study [10].
Sources and Search
The MEDLINE (through June 2019), Embase (through June 2019), and Cochrane Central Register of Controlled Trials databases, as well as the reference lists of the retrieved studies, were used to find trials that were relevant to the effects of TENS treatment in children on urodynamic indexes and objective OAB symptoms. We screened and included studies in our meta-analysis if the trials met the eligibility criteria. The search items were as follows: (ŌĆ£transcutaneous electric nerve stimulationŌĆØ or (ŌĆ£transcutaneousŌĆØ and ŌĆ£electricŌĆØ and ŌĆ£nerveŌĆØ and ŌĆ£stimulationŌĆØ) or ŌĆ£transcutaneous electric nerve stimulationŌĆØ or (ŌĆ£transcutaneousŌĆØ and ŌĆ£electricalŌĆØ and ŌĆ£nerveŌĆØ and ŌĆ£stimulationŌĆØ) or ŌĆ£transcutaneous electrical nerve stimulationŌĆØ) and (ŌĆ£urinary bladder, overactiveŌĆØ or (ŌĆ£urinaryŌĆØ AND ŌĆ£bladderŌĆØ and ŌĆ£overactiveŌĆØ) or ŌĆ£overactive urinary bladderŌĆØ or (ŌĆ£overactiveŌĆØ and ŌĆ£bladderŌĆØ) or ŌĆ£overactive bladderŌĆØ). Two authors independently screened the documents for inclusion. All disagreements were resolved by consensus of the authors.
Quality Assessment
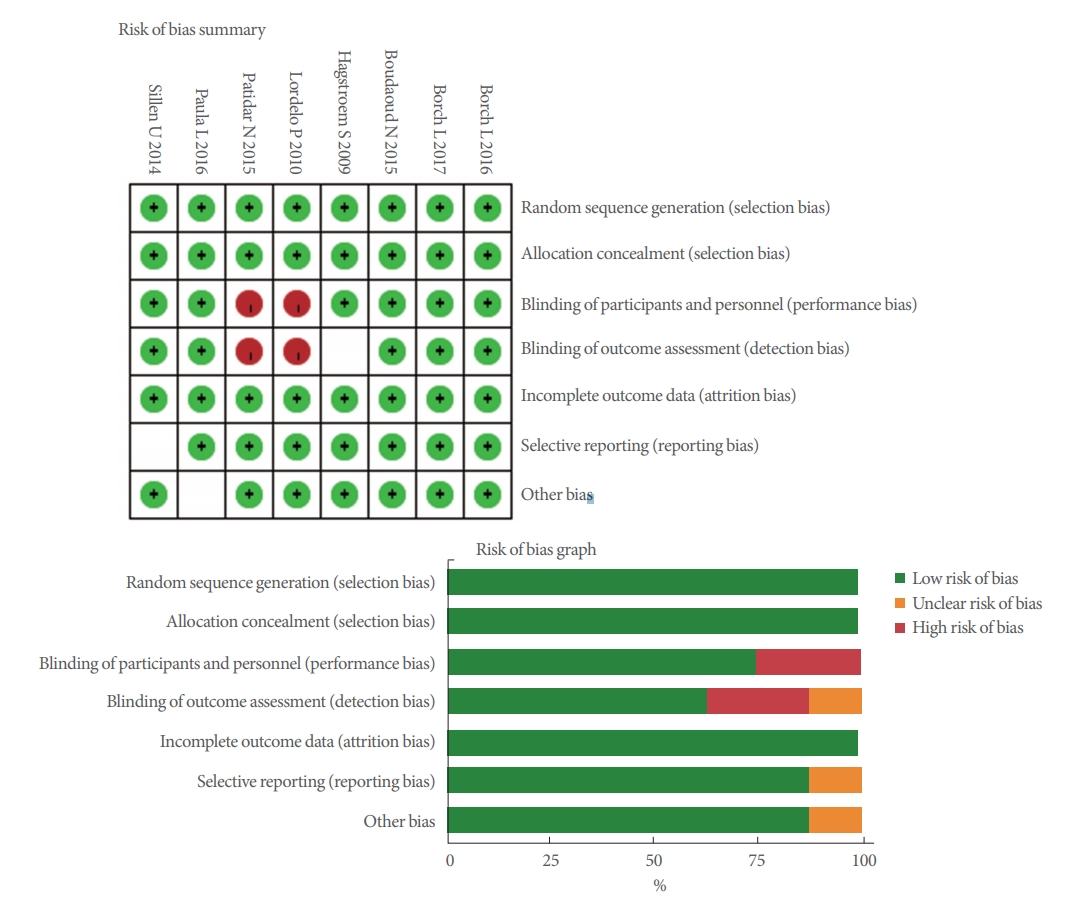
We used the Cochrane risk of bias tool [11] to evaluate the quality of each study. The quality items were selective outcome reporting, blinding, allocation concealment, incomplete outcome data, random sequence generation, and other sources of bias. A graph summarizing the risk of bias was generated based on discussions among the authors, as shown in Fig. 1. Then, individual studies were assessed in line with principles derived from the Cochrane Handbook for Systematic Reviews of Interventions v5.10 [12]. Every article was evaluated with a grade of A (satisfied almost all of the quality criteria), B (partially satisfied or fuzzy), or C (barely satisfied). All reviewers independently assessed whether each study fit the criteria, and then extracted the data from the selected studies.
Data Extraction
One author read the articles and extracted the following data: general information on the study (e.g., the name of the first author, publication date, country, and the study design), the characteristics of the patients (e.g., age), the interventions performed in the different groups (e.g., TENS or placebo, nerve stimulation scheme, and duration), and data on outcomes, including wet days/wk, visual analogue scale (VAS) scores, average voided volume (AVV), maximum voided volume (MVV), the number of patients with no response (or a partial or full response), daily voiding frequency, daily incontinence episodes, and daily number of voids. All the extracted data were checked by another author.
The main outcome of interest for this study was wet days/week. The secondary outcomes investigated to assess effectiveness were VAS scores, the numbers of patients with no response (or a partial or full response), daily voiding frequency, daily incontinence episodes, and daily number of voids. MVV and AVV were used as outcomes of urodynamic testing to assess the effectiveness of TENS treatment.
A VAS was used for pain assessment, in accordance with common practice in clinical medicine. The basic method is to use a scale with a length of about 10 cm, marked with 10 scale markers on one side, with the ends marked as ŌĆ£0ŌĆØ and ŌĆ£10,ŌĆØ respectively. On this scale, 0 refers to no pain, and 10 corresponds to the most severe (unbearable) pain.
Statistical Analysis and Meta-Analysis
RevMan ver. 5.1 [12] was used to perform a meta-analysis of continuous and dichotomous data. The mean difference (MD) with a 95% confidence interval (CI) [13] was employed to compare continuous data, while the odds ratio (OR) with a 95% CI was used to compare dichotomous data among various groups. The I2 test and Mantel-Haenszel chi-square test were employed to evaluate statistical heterogeneity; on this basis, we chose a fixed-effects model if P>0.05, and otherwise used a randomeffects model. This meta-analysis did not require ethical approval or patient consent, since all data were obtained from previously published articles.
RESULTS
Study Selection Process, Search Results, and Characteristics of the Trials
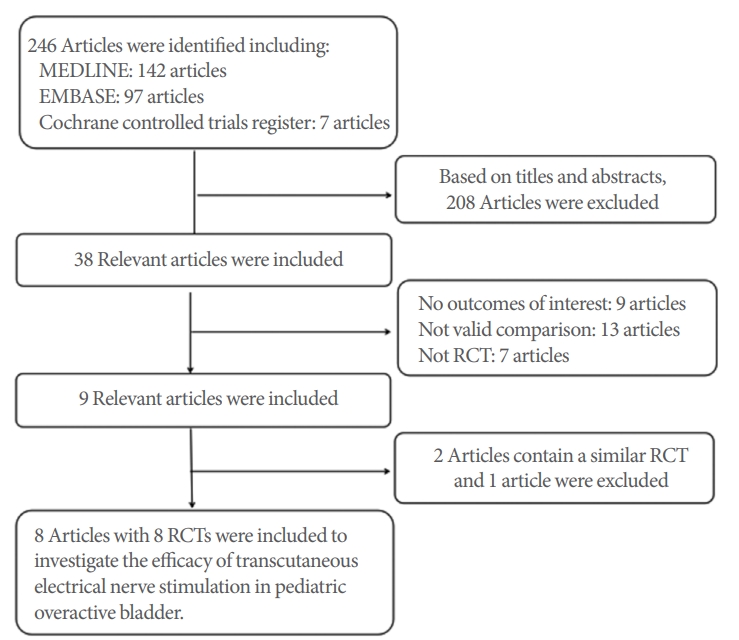
We found 246 papers by searching MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials databases. Of these papers, 208 were excluded based on the abstract according to the inclusion and exclusion criteria. Twenty-nine articles were excluded because they did not provide useful data, and 1 article was excluded because it described an experiment. Eight papers described RCTs [14-21] evaluating the effects of TENS treatment in children on urodynamic indexes and objective OAB symptoms. Details on the studies and characteristics of the patients are shown in Table 1. The study selection process is depicted in Fig. 2.
Risk of Bias in the Studies
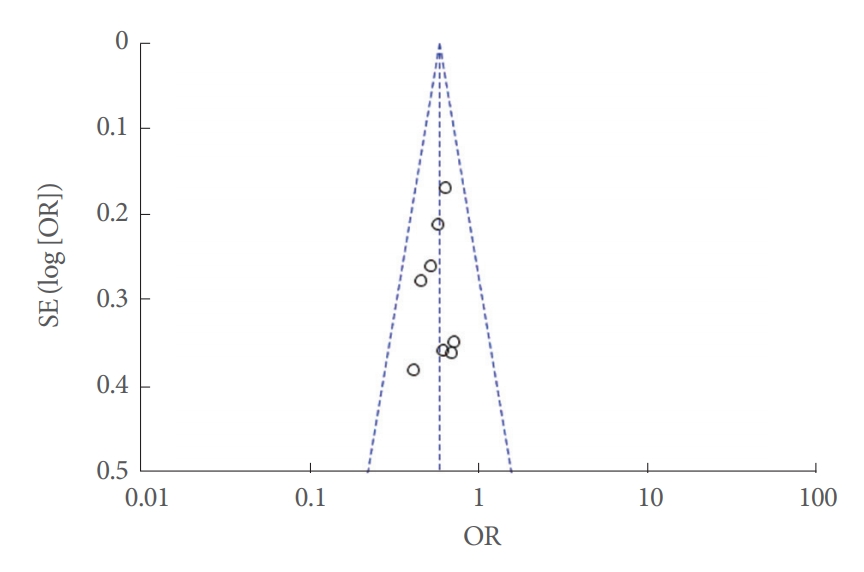
All 8 of the studies included in our meta-analysis followed a randomization process. Five papers [14,15,18,19] had an appropriate calculation of the number of patients. Two studies [19,20] did not specify a blinding protocol, with a Jadad score of B (Table 2). Fig. 1 presents a graphical summary of the risk of bias. No evidence of publication bias was found (Fig. 3). No uniform intervention period, frequency, intensity, pulse duration, or nerve stimulation scheme was found across the 8 studies (Table 1), and this variation automatically introduced considerable heterogeneity into the analysis. The quality assessment of individual studies is shown in Table 2.
Primary Outcomes
Wet days/week
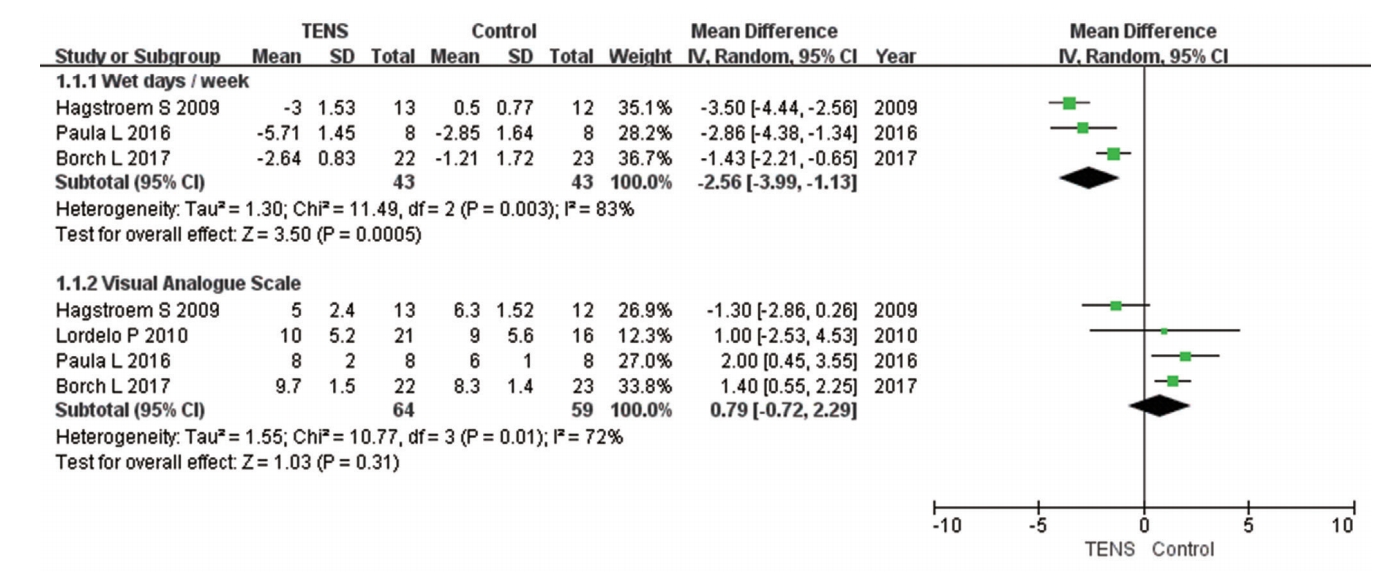
Three papers with 86 patients (TENS group, 43 patients; control group, 43 patients) reported data on wet days per week. As shown in Fig. 4, TENS led to a greater decrease in wet days per week (MD, -2.56; 95% CI, -3.99 to -1.13; P=0.0005).
Outcomes of Urodynamic Testing
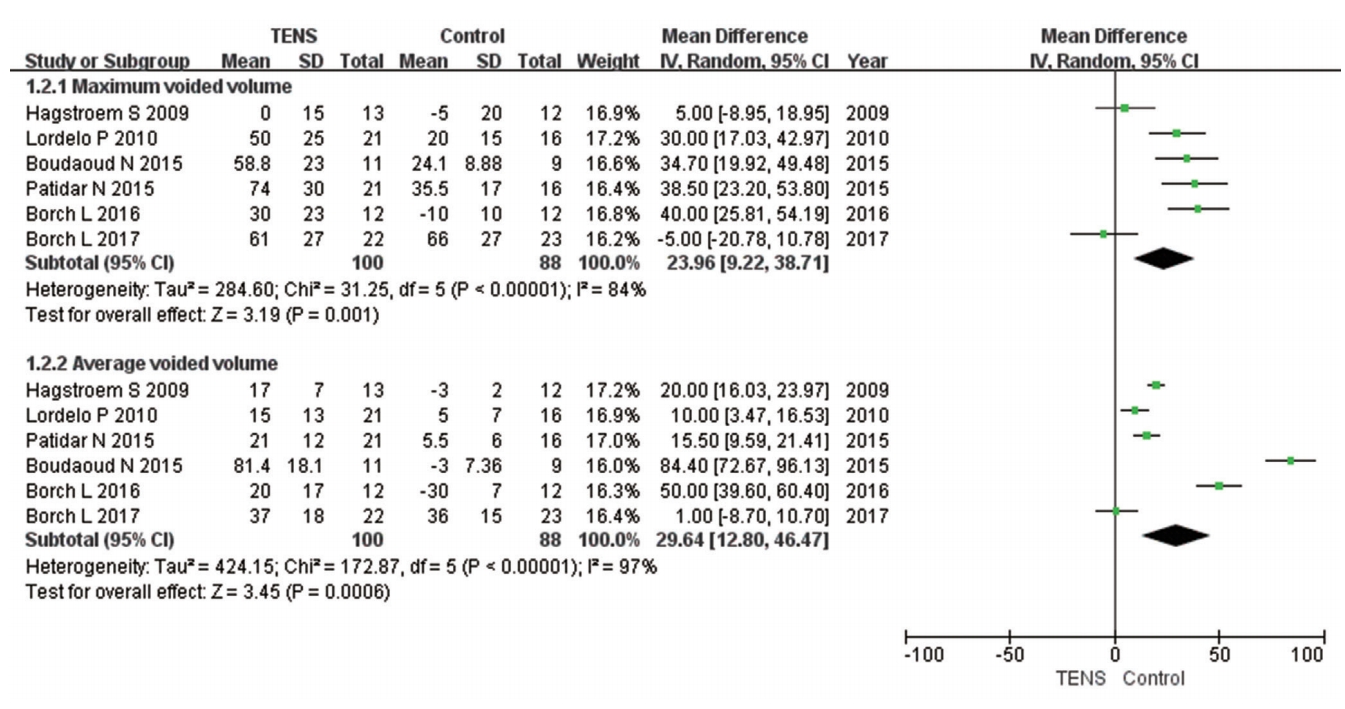
Maximum voided volume
Six papers with 188 patients (TENS group, 100 patients; control group, 88 patients) analyzed changes in MVV. A random-effects model showed a statistically significant difference in MVV (MD, 23.96; 95% CI, 9.22ŌĆō38.71; P=0.001) (Fig. 5). This result implies that MVV showed significant improvement after TENS treatment in pediatric OAB patients.
Average voided volume
Six papers with 188 patients (TENS group, 100 patients; control group, 88 patients) analyzed changes in AVV. A random-effects model showed a statistically significant difference in AVV (MD, 29.64; 95% CI, 12.80ŌĆō46.47; P=0.0006) (Fig. 5). This result implies that AVV showed significant improvement after TENS treatment in pediatric OAB patients.
Secondary Outcomes
Visual analogue scale scores
To evaluate changes in VAS scores, 4 RCTs with 123 patients (TENS group, 64 patients; control group, 59 patients) were analyzed. The MD was 0.79 (95% CI, -0.72 to 2.29; P=0.31) (Fig. 4). This result indicated that TENS treatment did not cause obvious pain and discomfort in pediatric OAB patients.
Numbers of patients with no response, a partial response, and a full response
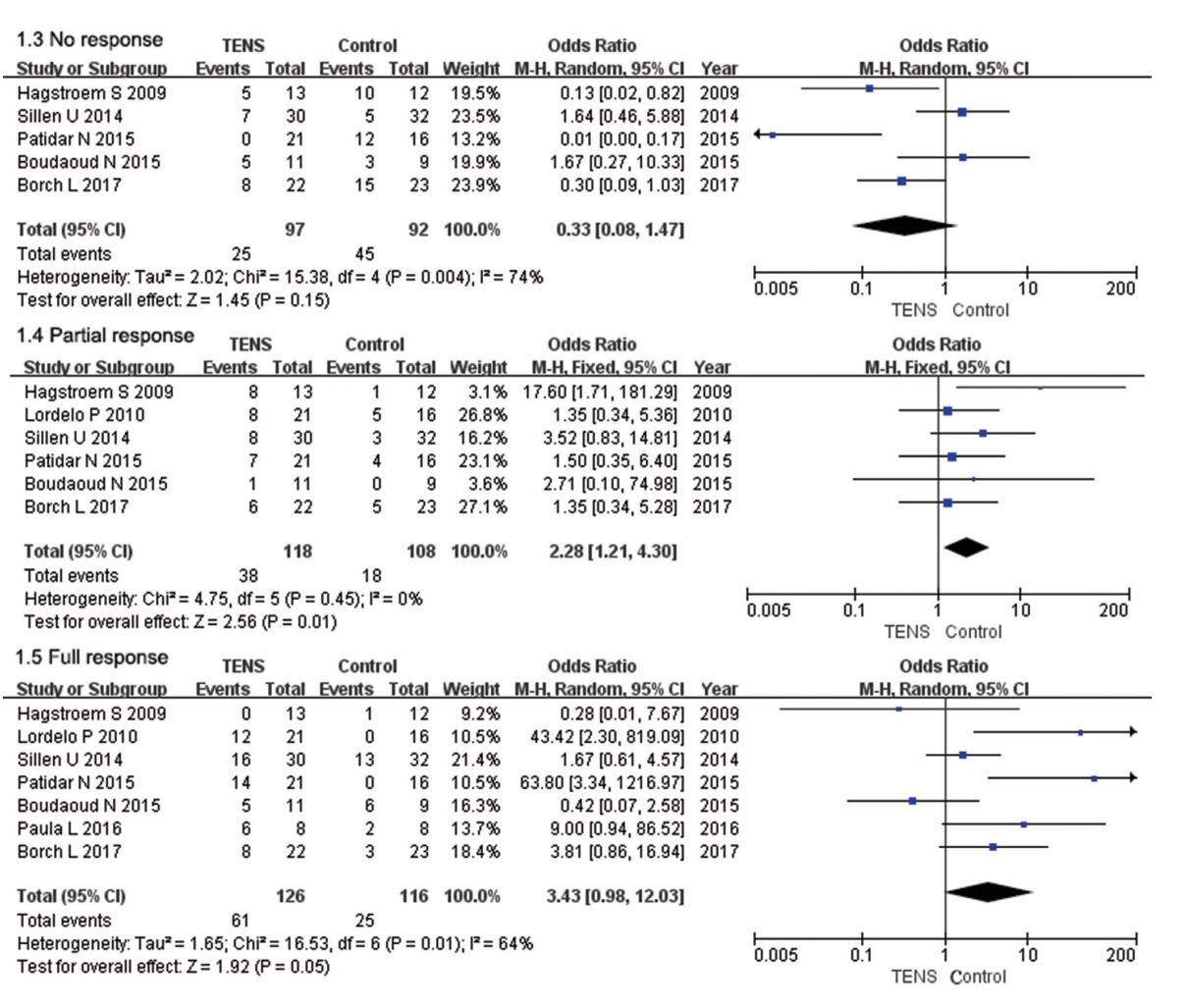
Five RCTs with 189 patients (TENS group, 97 patients; control group, 92 patients) included data on the number of patients with no response. There was no significant difference in the number of patients with no response (OR, 0.33; 95% CI, 0.08ŌĆō1.47; P=0.15) (Fig. 6).
Six RCTs with 226 patients (TENS group, 118 patients; control group: 108 patients) included data on the number of patients with a partial response. Forest plots showed that the TENS group had a larger number of patients with a partial response than the control group (OR, 1.35; 95% CI, 0.34ŌĆō4.30; P=0.01) (Fig. 6).
Six RCTs with 242 patients (TENS group, 126 patients; control group: 116 patients) included data on the number of patients with a full response. Forest plots showed no significant difference between the TENS and control groups in the number of patients with a full response (OR, 3.34; 95% CI, 0.98ŌĆō12.03; P=0.05) (Fig. 6).
Daily voiding frequency and daily incontinence episodes
Two RCTs enrolling 87 patients (TENS group, 43 patients; control group, 44 patients) contained data on daily voiding frequency and daily incontinence episodes. Forest plots showed that the TENS group had a visually notable reduction in daily voiding frequency (MD, -0.70; 95% CI, -1.00 to -0.41; P < 0.00001) and daily incontinence episodes (MD, -0.82; 95% CI, -1.16 to -0.47; P<0.00001) (Fig. 7).
Daily number of voids
Two RCTs included data on the daily number of voids in 74 patients (TENS group, 42 patients; control group, 32 patients). Forest plots showed that the TENS group had significantly fewer daily voids than the control group (MD, -3.16; 95% CI, -3.61 to -2.71; P<0.00001) (Fig. 7).
DISCUSSION
Over time, increasingly many studies have investigated the use of TENS to treat children clinically diagnosed with OAB, as it is considered to be an effective, noninvasive, and easy-to-use treatment modality [22]. It has a few reported side effects, such as skin reactions under adhesive electrodes, and very few contraindications, especially in children [23]. However, due to the limited number of children with OAB, large-scale data analysis still has yet to be conducted to establish the clinical and urodynamic criteria for the use of TENS to treat pediatric OAB.
We conducted this meta-analysis of 8 RCTs including 266 participants to evaluate the effects of TENS treatment in children on urodynamic indexes and objective OAB symptoms. Our study found that TENS led to a greater decrease of wet days/week (P=0.0005), daily voiding frequency (P<0.00001), daily incontinence episodes (P<0.00001), and daily number of voids (P<0.00001) compared with the control group. Furthermore, patients treated with TENS had similar VAS scores to patients in the control group, which showed that TENS treatment did not significantly increase patientsŌĆÖ discomfort and pain. Compared with the control group, TENS was relatively advantageous in terms of the number of patients with a partial response, but no obvious differences were found in the numbers of patients with no response or a full response. In urodynamic testing, TENS led to obvious improvements in MVV and AVV for children with OAB compared to the control group. In brief, TENS had an appreciable effect on the improvement of urodynamic indexes and objective OAB symptoms without a significant increase of pain and discomfort.
In Table 1, we summarized all RCTs and present the different parameters of electrical stimulation used to treat lower urinary tract symptoms in children. The parameters of electrical stimulation were clearly different across the studies, and the range of parameters was often wide. The frequency of electrical stimulation ranged from 10 to 20 Hz, but 2 studies [24,25] showed that a higher frequency of the current led to significant improvements in patientsŌĆÖ quality of life. Most studies reported a relatively consistent pulse duration of 200 ms, although this standard was not completely uniform. The intensity of electrical stimulation varied widely (up to 40 mA) and was defined in some studies as variable, depending on the tolerance of each child. However, previous studies on electrical stimulation of the bladder have shown that a shorter duration of electrical stimulation did not significantly change the process of contraction, and a lower frequency of electrical stimulation did not increase the effect of stimulation [26,27]. Different treatment regimens in terms of the frequency, duration of each treatment, and total duration of treatment seem to affect outcomes, giving the impression that the longer the treatment, the better.
Theoretically, the pathophysiological mechanism of detrusor overactivity is complicated, mainly due to the interaction of factors related to the peripheral nervous system and central nervous system [28]. Imbalances or interruptions of signals in regulatory pathways may lead to overactivity of the detrusor muscle. The mechanisms of the above neural regulatory pathways are not well understood [29]. Neuromodulation may lead to a rebalancing of the inhibitory and excitatory functions of the central nervous system, which controls the systolic and diastolic functions of the detrusor muscle of the bladder. Stimulation of the posterior tibial nerve results in depolarization of the afferent fibers of the sacral and lumbar vertebrae, which suppresses bladder contractile activity. Afferent stimulation, mainly by means of the direct pathway of the sacral cord, exerts a central inhibitory effect on preganglionic bladder motor neurons [30].
The immediate effect of electrical nerve stimulation is achieved by directly stimulating a nerve or muscle, which affects the process of nerve transmission within the context of nerve regulation, but no immediate response occurs in patients without neuropathologic dysfunction. Electrical stimulation of the lower urinary tract has been shown to induce chemical changes capable of increasing adrenergic reactions and leading to detrusor relaxation [31]. At the same time, electrical stimulation can also reduce cholinergic reactions, change the content of other neurotransmitters (e.g., nitric oxide and serotonin), and increase the content and concentration of endorphins or enkephalins in cerebrospinal fluid [31]. This may also explain why TENS did not increase pain and discomfort in patients with OAB compared with the control group.
Compared with adults, the theoretical advantage of electrical nerve stimulation in children lies in the greater plasticity of the central and peripheral nervous systems, which have the potential to be reshaped. A growing body of evidence suggests that lower urinary tract dysfunction in adults is intrinsic and longlasting, and electrical stimulation of the nerves therefore does not work as well as in children [32,33].
To summarize, TENS had a remarkable effect on the improvement of urodynamic indexes and objective OAB symptoms without a significant increase in pain and discomfort for children with OAB. In the future, TENS may become the mainstream treatment of children with OAB, and more large-scale clinical studies are needed to explore the safety of this method.
However, some limitations of our meta-analysis should be discussed. First, there was no uniform definition of the criteria used to determine the intervention period, frequency, intensity, pulse duration, or nerve stimulation scheme. Second, this meta-analysis only included 8 trials, with relatively few subjects. However, all of the included studies aligned with our inclusion criteria, and we are of the opinion that these limitations do not have a major impact on the results. Nonetheless, there is still a need for additional high-quality trials to provide more evidence.
In conclusion, TENS had a remarkable effect on the improvement of urodynamic indexes and objective OAB symptoms without a significant increase in pain and discomfort for children with OAB.