For Physicians Managing Voiding Dysfunction, Improving the Detection Rate of Early Prostate Cancer and Discrimination From Benign Prostatic Hyperplasia, in a Molecular Biomarker Aspects
Article information

Abstract
Prostate cancer (CaP) is the most common cancer diagnosed among men in the United States and the fifth most common cancer among men in Korea. Unfortunately, the early stages of CaP may have no symptoms. Thus, early detection is very important and physicians managing voiding dysfunction must have awareness about CaP. The traditional tests used for early detection of CaP are the prostate-specific antigen (PSA) blood test and digital rectal examination. However, a high PSA level is not specific for CaP. Benign prostatic hyperplasia, prostatitis, urinary tract infection, and urinary retention can all cause a high PSA level. Thus, no test shows sufficient accuracy to truly be useful for screening men for CaP. A prostate biopsy is the only method that yields a definitive diagnosis of CaP; however, this test is invasive and uncomfortable. Recently, new biomarkers for CaP detection have been proposed to improve the accuracy of the PSA test. In this review, we summarize our knowledge of various new biomarkers, including PSA-associated biomarkers (the prostate health index and 4Kscore), molecular biomarkers (PCA3, TMPRSS2: ERG fusion gene, and various miRNAs), and proteomics-associated biomarkers, and the ways in which they may improve the detection rate of CaP. Accordingly, this review can raise awareness about CaP to physicians managing voiding dysfunction and be a good reference for them.
INTRODUCTION
Prostate cancer (CaP) is the most common cancer diagnosed among men in the United States, with an estimated 164,690 new cases and 29,430 deaths expected in 2018 [1]. In Korea, CaP was the fifth most common cancer among men in 2015, although the incidence is increasing rapidly [2]. The Korea National Cancer Incidence database shows that about 1,400 cases were diagnosed in 1999 and about 9,000 in 2011 [3].
Unfortunately, there may be no symptoms at the early stage of CaP. Accordingly, frequency, nocturia, dysuria, hematuria, weak stream, and pain might develop at the later stages. Thus, early detection of CaP is very important as it can improve survival rates significantly [4]. The traditional tests for early detection of CaP are the prostate-specific antigen (PSA) test and digital rectal examination (DRE). For a long time, the serum PSA test was used widely as a screening test for CaP. Gann et al. [5] reported that the sensitivity of the test for CaP during a 10-year follow-up of 22,071 men aged 40–84 years was 46% at a cutoff of 4.0 ng/mL. However, high PSA levels are not specific to CaP. Benign prostatic hyperplasia (BPH), prostatitis, urinary tract infection, and urinary retention can all cause high PSA levels [5-7]. Thus, no test has sufficient accuracy to reliably screen populations of men for CaP. A prostatic biopsy is the only method that yields a definitive diagnosis of CaP.
Recently, interest in new CaP biomarkers or methods of detection has increased; the aim being to improve the accuracy of the PSA test. In this review, we discuss new biomarkers that may improve the detection rate of CaP and discriminate it from BPH.
PSA-ASSOCIATED BIOMARKERS
The Prostate Health Index
PSA is a glycoprotein that binds to protease inhibitors and circulates in the blood. Only a small amount of PSA is not bound to protein; this is called free PSA (fPSA). The percentage of fPSA to total PSA (%fPSA) is significantly lower in patients with CaP than in those without. fPSA comprises three isoforms: proPSA, benign PSA, and intact PSA. The [-2]proPSA isoform is the most stable form of proPSA (referred to as p2PSA). In June 2012, the U.S. Food and Drug Administration (US FDA) approved the prostate health index (PHI) for clinical use. The test was used to detect CaP in men aged >50 years with a PSA level between 4 and 10 ng/mL and nonsuspicious DRE results. The formula for the PHI is (p2PSA/fPSA)×√total PSA [8]. A meta-analysis revealed that the PHI may reduce the number of unnecessary biopsies and be better at detecting CaP than total PSA and %fPSA, with an area under the curve (AUC) from 0.703–0.77 [9]. Another meta-analysis of PHI conducted for men with PSA levels in the “gray” area reported that the PHI and %fPSA were 0.74 and 0.63, respectively. In addition, a meta-regression analysis confirmed the superiority of PHI, which showed a relative diagnostic odds ratio of 2.81 compared with %fPSA [10]. Finally, another study showed that the PHI has a sensitivity of 0.89 and a specificity of 0.34 for detecting CaP. The sensitivity for detecting high grade CaP was 0.93 and the specificity was 0.34 [11].
The 4Kscore
The 4Kscore is a commercial test from Opko Diagnostics. The panel combines total PSA, fPSA, iPSA, and human kallikrein 2 (a glycoprotein). When used alongside DRE, the panel demonstrated very good diagnostic performance for detecting high grade CaP with Gleason score ≥7, with high AUCs [12]. However, the 4Kscore was not approved by the US FDA.
MOLECULAR BIOMARKERS
PCA3
The prostate cancer gene 3 (PCA3) was identified in 1999; this gene is expressed at much higher levels in CaP tissue than in non-neoplastic tissue [13]. Use of the PCA3 test for post-DRE urine samples was approved by the US FDA in 2012. Clinicians use the information to decide whether to repeat a prostate biopsy in men with negative biopsy results on a previous biopsy. PCA3 was more accurate than the PSA test for predicting clinically significant CaP, thereby improving the accuracy of CaP detection. Filella et al. [14] suggest that PCA3 is particularly useful for selecting patients in whom a biopsy should be repeated when the first biopsy was negative, and for detection and management of early CaP. A recent meta-analysis of case control studies revealed that the sensitivity, specificity, and AUC of the urine PCA3 test were 0.65, 0.73, and 0.75, respectively [15]. Thus, the urine PCA3 test has acceptable sensitivity and specificity for the diagnosis of CaP and can be used as a noninvasive method for that purpose. However, the cutoff value that yields the best discrimination is unclear [16].
TMPRSS2: ERG Gene Fusion Biomarkers
Gene fusions result from a combination of 2 or more separate genes to form a single chimeric gene or transcript; such fusions are an important driver of cancer. Genomic rearrangements are a major mechanism that drives prostate carcinogenesis [17]. TMPRSS2: ERG is the most common gene rearrangement found in CaP [18].
The TMPRSS2: ERG fusion gene can be detected in urine samples obtained after prostate massage. Calculation of the TMPRSS2: ERG mRNA/PSA mRNA ratio yields the TMPRSS2: ERG score. Combination of the TMPRSS2: ERG and PCA3 scores has been proposed as a way to improve prediction of whether a biopsy will detect CaP. Combined analysis of TMPRSS2: ERG and PCA3 allows detection of CaP with a diagnostic accuracy of 84%, which is significantly higher than that of the PSA test [19]. A prospective multicenter study by Leyten et al. [16] reported that TMPRSS2: ERG independently improved the predictive value of PCA3 for CaP.
Tissue miRNAs as Biomarkers
miRNAs are small RNAs (20 to 22 nucleotides in length) that modulate important cellular processes/pathways that contribute to cancer. Several studies have examined differences in expression of miRNAs between CaP and adjacent tissues [20-23]. Zhu et al. [20] reported that expression of miR-30c and miR-29b in CaP tissues was significantly lower than that in adjacent tissues. Feng et al. [21] found that tissue miR-17-92 could discriminate patients with CaP from those with BPH, making it a potential diagnostic biomarker for CaP; also, combination of the miR-17-92 cluster and serum PSA levels may increase the accuracy of CaP diagnosis. Paziewska et al. [22] showed differential expression of miR-187-3p, miR-183-5p, miR-32-5p, and miR-141-5p between BPH and CaP tissues; they also suggested that these miRNAs can differentiate between nonmalignant and malignant prostate tissue even when no neoplastic cells are detected in a biopsy specimen. We reported previously that expression of hsv1-miR-H18 and hsv2-miR-H9-5p was significantly higher in CaP tissues than in surrounding noncancerous tissues, and suggested that hsv1-miR-H18 and hsv2-miR-H9-5p might be associated with tumorigenesis in the prostate [23].
Blood miRNAs as Biomarkers
Circulating miRNAs are highly stable in the circulation; therefore, they may be useful biomarkers for improving disease diagnosis [24]. Several studies have been conducted to discriminate CaP from BPH [24-28]. Dybos et al. [25] reported that serum miR-148-3p is higher in men with CaP than in healthy controls and also located in prostate tissue. Al-Kafaji et al. [24] found that levels of miR-15a, miR-126, miR-192, and miR-377 were significantly lower in blood samples from CaP patients than in those from individuals with BPH or those from healthy patients. Receiver operating characteristic curve analysis revealed that miRNAs distinguished patients with CaP from those with BPH. Porzycki et al. [26] reported that miR-141-3p, miR-21, and miR-375 were expressed at higher levels in a CaP group than in a healthy control group; miR-375 showed an AUC value of 0.906. Tinay et al. [27] showed that expression of miR-345-5p was much higher in serum from CaP patients than in that serum from individuals without cancer, whereas Matin et al. [28] showed that miR-152-3p was elevated in plasma of CaP patients (AUC=0.88) and has the potential to improve early CaP diagnosis. However, McDonald et al. [29] reported that, after adjusting for age and P-values, no miRNAs in plasma were associated with a diagnosis of CaP. Thus, further studies are needed to identify miRNAs in blood that are suitable for CaP diagnosis.
Urine miRNAs as Biomarkers
Urinary miRNAs may be useful diagnostic markers. Many studies show the utility of urinary miRNAs [30-34]. For example, Bryant et al. [30] found that miR-107 and miR-574-3p were present in urine from CaP patients at significantly higher concentrations than in urine from controls. Rodríguez et al. [31] reported downregulation of miR-196a-5p and miR-501-3p in urinary exosomes from CaP patients, and suggested that these might serve as noninvasive biomarkers for CaP. Korzeniewski et al. [32] found that patients with CaP express higher levels of miR-483-5p in the cell-free urine fraction than control patients, whereas Lewis et al. [33] reported that expression of miR-888 in EPS urine was higher in CaP patients with high grade disease than in those with low grade disease. Srivastava et al. [34] found that imR-205 and miR-214 were significantly downregulated in urine from CaP patients, and that these miRNAs can discriminate CaP patients from healthy individuals with 89% sensitivity and 80% specificity. However, the methods used for quantitation and normalization in these studies were not standardized. Whereas most studies used urine sediment, others used supernatant or cell-free urine. Also, some samples were obtained after prostate massage and others were not. miRNA biomarkers for CaP were summarized in Table 1.
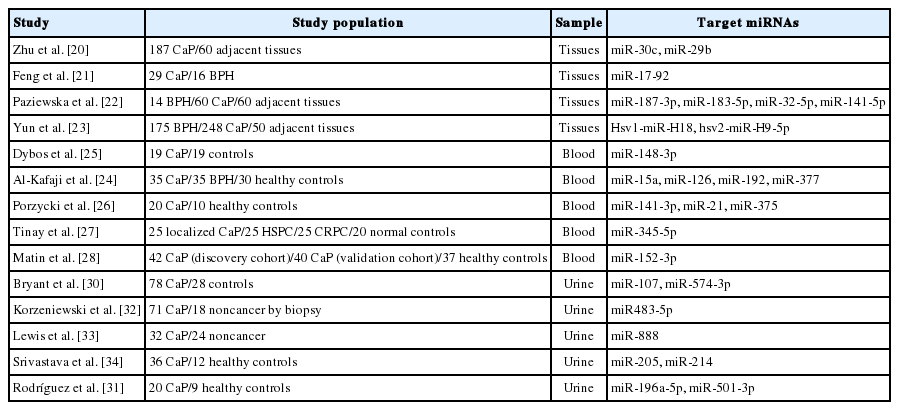
Studies to identify miRNA biomarkers for CaP
PROTEOMICS-ASSOCIATED BIOMARKERS
Proteomics offers useful tools for identifying and quantifying novel protein biomarkers. Urine is one of the most attractive bio-fluids for clinical proteomics analysis. Below, we summarize studies based on gas chromatography (GC) or liquid chromatography (LC)-mass spectrometry (MS). Proteomics biomarkers for CaP were summarized in Table 2.
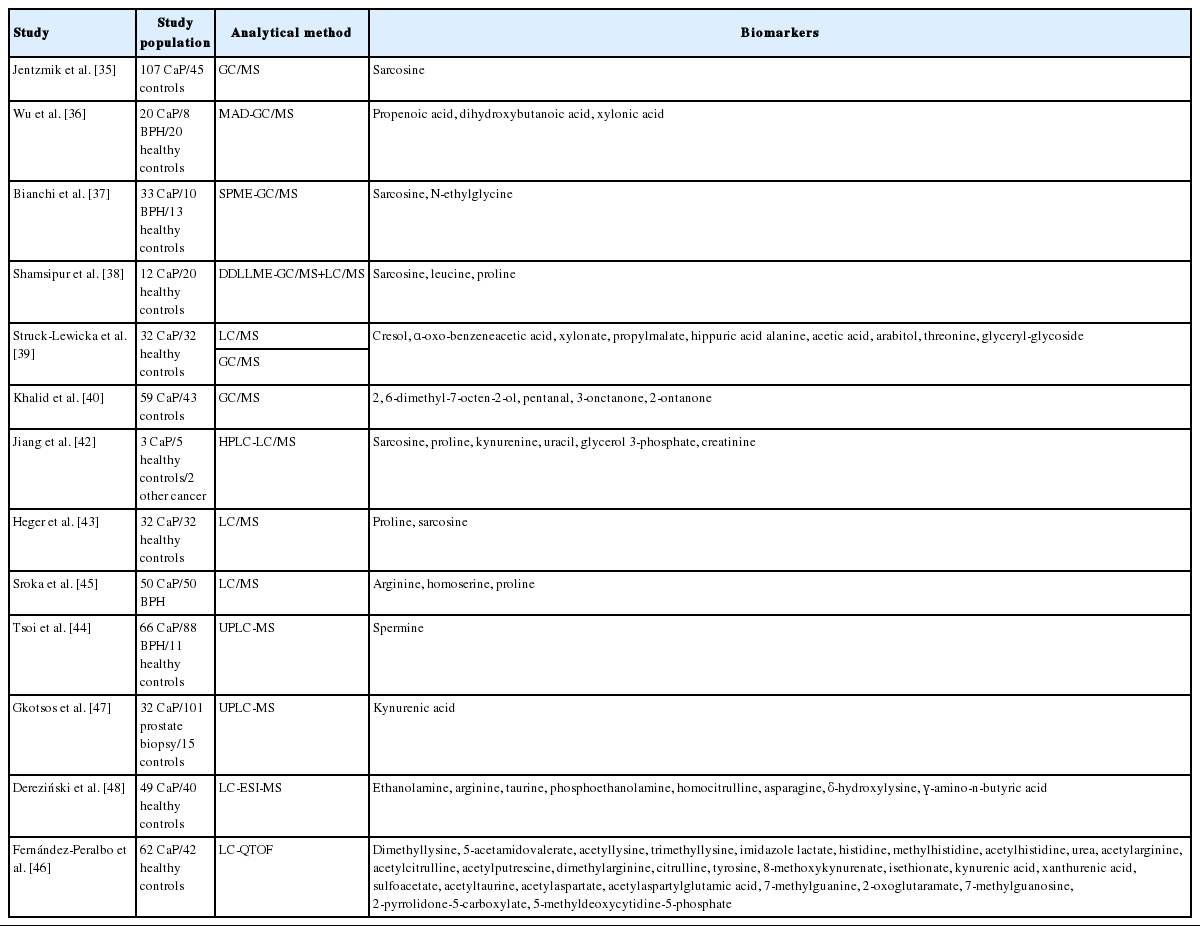
CaP biomarkers proposed by proteomics studies
GC-MS
GC-MS is an analytical method that combines the features of gas chromatography and mass spectrometry to identify different substances within test samples. Many studies have used GC-MS to identify new protein biomarkers [35-40]. Jentzmik et al. [35] reported that the median sarcosine-creatinine ratio in urine was 13% lower in CaP patients (n=107) than in controls (n=45), and that sarcosine detected in urine after DRE was not a marker for detection of CaP or aggressive tumors. Wu et al. [36] used microwave-assisted derivatization together with GC/MS to obtain urinary metabolomics information from 20 CaP patients and compared it with information from eight BPH patients and 20 healthy men. There was no difference between the CaP group and the control groups in terms of urinary sarcosine levels. However, levels of propenoic acid, dihydroxybutanoic acid, and xylonic acid were significantly higher in the CaP group; these were suggested as biomarkers for CaP. Bianchi et al. [37] developed and validated a solid-phase microextraction-fast GC/MS method for direct measurement of sarcosine and N-ethylglycine in urine from CaP patients. They reported that sarconine may be a urinary biomarker for CaP, with 79% sensitivity and 87% specificity. Shamsipur et al. [38] proposed that combined measurement of sarcosine, leucine, and proline may reveal candidate biomarkers for CaP. They showed that urinary sarcosine levels in CaP patients were higher than those in controls, while urinary leucine levels were lower. Struck-Lewicka et al. [39] used GC-MS to show that alanine, acetic acid, arabitol, threonine, and glyceryl-glycoside were lower in CaP patients. Khalid et al. [40] investigated volatile organic compounds emanating from urine samples and identified four: 2,6-dimethyl-7-octen-2-ol, pentanal, 3-onctanone, and 2-ontanone. Pentanal levels were higher in CaP patients, while the levels of the other three were lower, than in healthy controls.
LC-MS
LC is a pressure-driven liquid-based separation method in which analytes are separated according to their adsorption/desorption kinetics. When coupled with MS, this technique provides high-efficiency separation and identification during a single analysis [41]. Several reports have used LC-MS to identify protein biomarkers for CaP [39,42-48]. Jiang et al. [42] developed a novel method (high performance liquid chromatography/MS) for detecting 6 compounds (sarcosine, proline, kynurenine, uracil, glycerol 3-phosphate, and creatinine) in urine samples that may show potential with respect to CaP screening. Struck-Lewicka et al. [39] used LC-MS to show that cresol, aoxo-benzeneacetic acid, xylonate, propylmalate, and hippuric acid were downregulated in urine of CaP patients. Heger et al. [43] investigated various urine parameters in CaP patients and healthy controls. They found that levels of urinary sarcosine and proline were high in CaP patients but absent from control samples. Tsoi et al. [44] used ultra-high performance LC-MS to evaluate the potential of urinary polyamines, putrescine, spermidine, and spermine as CaP biomarkers. Spermine demonstrated good diagnostic performance when discriminating between patients with CaP and those with BPH, making it a potential novel biomarker for CaP. Sroka et al. [45] revealed that arginine, homoserine, and proline were more abundant in urine samples from CaP patients; also, sarcosine was not a definitive indicator of CaP when analyzed in urine samples collected either before or after prostate massage. Fernández-peralbo et al. [46] found that 27 metabolites were present at lower concentrations in urine of CaP patients than in controls, while 7-methylguanine levels were higher in CaP patients. A connection between biochemical pathways (e.g., DNA methylation, epigenetic markers on histones, and RNA cap methylation) could explain the changes in the concentrations of potential biomarkers in individuals with CaP. Gkotsos et al. [47] observed that the median levels of sarcosine and kynurenic acid were lower, and those of uracil were higher, in CaP patients. Kynurenic acid was identified as a promising urine biomarker for CaP, while sarcosine and uracil were not significant. Finally, Dereziński et al. [48] showed that metabolic pathways associated with ethanolamine, arginine, and branched-chain amino acids could be a valuable source of markers for CaP; they also suggested that these metabolites might play a role in pathogenesis of CaP.
FUTURE PERSPECTIVES
Over the last 30 years, diagnosis of CaP has evolved markedly, and mortality related to CaP has fallen. The use of the PSA test as a screening tool has likely been a major contributor to this decrease. However, PSA is of limited use; therefore, interest in new biomarkers for CaP has increased. Over the past few decades, many potential CaP biomarkers have been suggested, but, they have not been used in a real practice. It might be lack of follow-up validation studies or failed to validate the previous studies. That might be cost effectiveness, technical problems, or wrong target biomarkers. The lack of follow-up validation studies means that research into CaP biomarkers is still at the discovery stage. Thus, many large cohort studies are needed to validate CaP biomarkers. Although none of the potential biomarkers identified to date have been translated into the clinic as replacements for the PSA test, the search for novel biomarkers (and validation of developed biomarkers in large cohorts) will continue. Technical development could solve these problems in the future.
Recently, the Stockholm3 test, which uses a combination of plasma protein biomarkers, genetic markers, clinical variables, and a prostate exam, was reported [49]. This test identified aggressive cancer in men with PSA levels as low as 1–3 ng/mL. SelectMDx is a biomarker that help a physician determine if a patient is at higher or lower risk for CaP and which men can safely avoid biopsy. Patients may benefit from a biopsy and early CaP detection or can avoid a biopsy and return to routine screening with biomarkers (DLX1 and HOXC6) and clinical risk factors (age, PSA, prostate volume, family history, and DRE) [50]. ConfirmMDx is a tissue test to improve the identification of men at risk for undetected clinically significant prostate cancer. ConfirmMDx could help identify men that may not need a repeat prostate biopsy with biomarkers (DNA meylation of GSTP1, RASSF1, and APC) and clinical risk factors [51]. Therefore, a combination of molecular biomarkers and clinical variables might be more appropriate for predicting early stage CaP.
CONCLUSIONS
Until now, there has been many efforts to predict early stage CaP such as PSA associated markers, various molecular markers, miRNA markers, and protein markers. Unfortunately, the follow-up validation studies are lack due to several reasons. Therefore, future studies of CaP biomarkers need to focus on combinations of molecular biomarkers and clinical variables, rather than on biomarkers alone.
Notes
Grant/Fund Support
This work was supported by the International Science and Business Belt Program through Ministry of Science, ICT and Future Planning (2017K000490).
Conflict of Interest
No potential conflict of interest relevant to this article was reported.