The Overactive Bladder Symptom Score, International Prostate Symptom Score–Storage Subscore, and Urgency Severity Score in Patients With Overactive Bladder and Hypersensitive Bladder: Which Scoring System is Best?
Article information

Abstract
Purpose
To evaluate the correlations among the Overactive Bladder Symptom Score (OABSS), International Prostate Symptom Score–Storage Subscore (IPSS-S), and the modified Urgency Severity Scale (USS) in patients with overactive bladder (OAB) and hypersensitive bladder (HSB) and to identify the most useful diagnostic tool for classifying the severity of OAB.
Methods
We retrospectively reviewed the charts of consecutive patients with OAB who visited our urologic clinics for treatment. All patients underwent a detailed history, physical examination, urinalysis, uroflowmetry, and postvoid residual volume measurement, and completed a 3-day voiding diary. All patients answered the Chinese versions of the IPSS, OABSS, and USS, according to which they were classified as having wet or dry OAB based on whether their chief complaint was urgency urinary incontinence or urgency without incontinence. HSB was defined as a functional bladder capacity <350 mL and a USS of 0 or 1.
Results
The records of 325 OAB patients (99 women and 226 men) were reviewed. The OAB subgroups included HSB (n=31), OAB-dry (n=74), and OAB-wet (n=220). One-way analysis of variance showed significant differences among the OAB subgroups evaluated using each scoring system. Each scoring system was significantly correlated with the OAB subgroups. The Spearman rho was 0.983 for the USS, 0.651 for the OABSS, and 0.428 for the IPSS-S.
Conclusions
The IPSS-S, OABSS, and USS showed good correlations with the OAB subgroups. Their ranking in terms of discriminant ability for classifying OAB severity as HSB, OAB-dry, and OAB-wet was USS>OABSS>IPSS-S. The simplest survey, the USS, with a single item scored from 0 to 4, had the strongest correlation with the OAB severity subgroups.
INTRODUCTION
Overactive bladder (OAB) is defined as a symptom syndrome of urinary urgency, with or without urgency incontinence, usually with urinary frequency, and nocturia, in the absence of infection or other obvious pathological features [1,2]. Patients are classified as having OAB-wet or OAB-dry based on whether their chief complaint is urgency frequency with or without urgency urinary incontinence (UUI), respectively. Urgency is defined as the core symptom of OAB. However, the word “urgency” and its definition have been the source of much debate and confusion. Yamaguchi et al. [3] conducted a “patient trust study” in 21 intelligent (i.e., to be “trusted”) female patients with OAB. The results showed that in 43% of patients seeking medical care, urgency episodes occurred less than once per day, and some patients had days without urgency. They hypothesized that OAB may be more accurately defined as hypersensitive bladder (HSB), rather than as a syndrome characterized by urgency. Increased bladder sensitivity or hypersensitivity appears to be the basis for inducing urgency. Lee et al. [4] also reported that bladder sensory profiles indicated that OAB patients had more sensitive bladders than non-OAB subjects. They concluded that the bladders of OAB patients may be not only overactive, but also hypersensitive. In clinical practice, HSB and OAB symptoms usually overlap, and patients with HSB might be classified as having dry OAB [5,6].
HSB, OAB-dry, and OAB-wet represent the spectrum of OAB severity. Wet OAB is usually considered to be the most severe subtype of OAB, UUI is stressful in terms of the physical and psychological ability to cope with the requirements of daily life and has a strong negative impact on the quality of a patient’s life [7,8]. In a large population-based cross-sectional study, Agarwal et al. [9] reported that urinary urgency was the most common troubling symptom. However, for individuals, urgency incontinence was the most likely to be rated as bothersome. UUI is associated with numerous comorbid conditions and inflicts a substantial personal burden on many aspects of patients’ lives, such as an increased risk for falls and fractures, depression, and problems with sexual function [8]. Patients with wet OAB make more adaptation efforts in daily living than patients with dry OAB [10,11].
OAB is defined by subjective symptoms, rather than objective measures. The patient’s perspective is the key point for the management of OAB. Several patient-reported questionnaires have been developed to characterize patients’ symptoms and their impact on quality of life [12,13]. Some of these questionnaires include the Overactive Bladder Questionnaire, Patient Perception of Bladder Condition [14], the Primary OAB Symptom Questionnaire, Overactive Bladder Symptom Composite Score, Urgency Questionnaire, and the Overactive Bladder Symptom Score (OABSS) [15]. Additionally, bladder diaries can provide a detailed record of information regarding OAB symptoms [16]. Nonetheless, keeping such a diary is inconvenient for some patients.
In our daily practice, we have used several different questionnaires to characterize lower urinary tract symptoms. This raises the question of which questionnaire is the best for determining the severity of OAB. The aim of this study was to evaluate the correlations among the International Prostate Symptom Score–Storage Subscore (IPSS-S) [17,18], the OABSS [19], and the Urgency Severity Scale (USS) [20] in patients with OAB and HSB and to identify the most useful diagnostic tool for classifying the severity of OAB.
MATERIALS AND METHODS
We retrospectively reviewed the charts of consecutive patients who complained of storage symptoms and visited our urologic clinic for treatment. As routine practice, all patients underwent a detailed clinical evaluation including a history, physical examination, urinalysis, urine culture, uroflowmetry, and postvoid residual volume measurement and completed a 3-day voiding diary recording urgency and UUI episodes. Additionally, all patients responded to the validated Chinese version of IPSS, which included a quality-of-life index, the OABSS, and the USS. An expert nurse carefully instructed the patients on the voiding diary and administered the questionnaires.
The study inclusion criteria were an age of 18 years or more and the ability to complete the serial evaluation measures. Patients with concomitant urinary tract infections, possible neurogenic lesions, urothelial carcinoma, and severe cardiovascular disease were excluded from the study. This study was approved by the Research Ethics Committee of the Buddhist Tzu-Chi General Hospital (TCGH IRB 098-38). Wet OAB was considered to be present if the 3-day voiding diary revealed at least 1 episode of UUI. Dry OAB was suspected when the voiding diary showed no UUI episode but at least 1 urgency episode. HSB was considered to be present when there was no urgency episode in the voiding diary, but the patient’s functional bladder capacity was less than 350 mL. An average voiding frequency of fewer than 8 times per day and a functional bladder capacity of more than 350 mL were considered normal.
The IPSS is composed of 7 questions investigating storage symptoms (questions 2, 4, and 7) and voiding symptoms (questions 1, 3, 5, and 6). The storage subscore ranges from 0 to 15, the voiding subscore ranges from 0 to 20, and the total score ranges from 0 (no symptoms) to 35 (maximal symptoms). A quality-of-life index, with a scale of 0–6 (delighted to terrible), is also included in the IPSS [18].
The OABSS is a symptom assessment questionnaire designed to quantify OAB symptoms into a single score [19,21]. The questionnaire consists of 4 questions on OAB symptoms with maximum scores ranging from 2 to 5: daytime frequency (2 points), night-time frequency (3 points), urgency (5 points), and UUI (5 points). The total score ranges from 0 to 15 points, with higher scores indicating higher symptom severity.
The validated Chinese version of the USS questionnaire is a modified version of the Indevus Urgency Severity Scale (IUSS) [20]. The USS differs from the IUSS because urine leakage is included in the 3 other urgency scales. The USS is scored as 0 (no feeling of urgency), 1 (mild urgency), 2 (moderate urgency), 3 (severe urgency), or 4 (inability to hold urine). We used the validated Chinese version of the USS to distinguish true urgency (USS=2, 3, or 4) from strong urge to void (USS=0 or 1) for patient selection (Table 1). The USS was administered to all patients by a well-trained nurse who explained the meaning of urgency. The USS questionnaire was validated in terms of test-retest reliability and correlated with a Chinese version of the OABSS to assess its feasibility for patient acceptance and detecting clinical responsiveness to antimuscarinic therapy [22]. The sensation of urgency was defined as the sensation of a strong desire to void that was difficult to defer. When a patient had even a single drop of urine leakage in association with a strong urgency sensation, UUI was considered to have occurred.

Urgency Severity Scale questionnaire
The statistical analysis was performed using IBM SPSS Statistics ver. 20.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as means±standard deviations and categorical data are given as numbers (n) and percentages (%). Statistical comparisons between the groups were made using 1-way analysis of variance (ANOVA) with multiple comparisons and the Spearman correlation coefficient rho (ρ) with a subsequent significance test. We described the strength of the correlation using the following guide for the absolute value of rho (ρ): very weak (0.00–0.19), weak (0.20–0.39), moderate (0.40–0.59), strong (0.60–0.79), and very strong (0.80–1.00). P-values less than 0.05 were considered to indicate statistical significance.
Receiver operating characteristic (ROC) curve analysis was also performed to determine the value of the questionnaire as a diagnostic tool. Using Hosmer and Lemeshow’s rule for logistic models, the discriminative abilities of the models were classified according to the area under the ROC curves (AUC or AUROC) as poor (0.5≤AUC<0.7), acceptable (0.7≤AUC<0.8), excellent (0.8≤AUC<0.9), or outstanding (AUC≥0.9) [23]. Comparisons of the AUROC values for each scoring system in each subgroup of OAB were also made.
RESULTS
A total of 325 OAB patients were recruited, including 99 women and 226 men. Their mean age was 72.6±12.0 years (female, 68.5±13.7 years and male, 74.4±10.8 years). Thirty-one patients (9.5%) had HSB, 74 (22.8%) had OAB-dry, and 220 (67.7%) had OAB-wet. Table 2 and Fig. 1 show the USS, OABSS, and IPSS-S scores for each of the OAB subgroups (HSB, OAB-dry, and OAB-wet). The scores of each of the questionnaires progressively increased as severity increased from HSB to OAB-dry and OAB-wet. One-way ANOVA showed significant differences among the OAB severity subgroups evaluated with each scoring system (all P<0.001). Multiple comparisons also indicated significant differences among each of the 3 OAB severity subgroups evaluated with each scoring system (all P<0.05). Post hoc tests for the USS yielded results of P<0.001 for all comparisons of OAB subgroups; for the OABSS, P=0.002 for HSB versus OAB-dry and P<0.001 for the other comparisons; and for the IPSS-S, P=0.030 for HSB versus OAB-dry and P<0.001 for the other comparisons.

Comparisons of USS, OABSS, and IPSS-S scores among the OAB subgroups
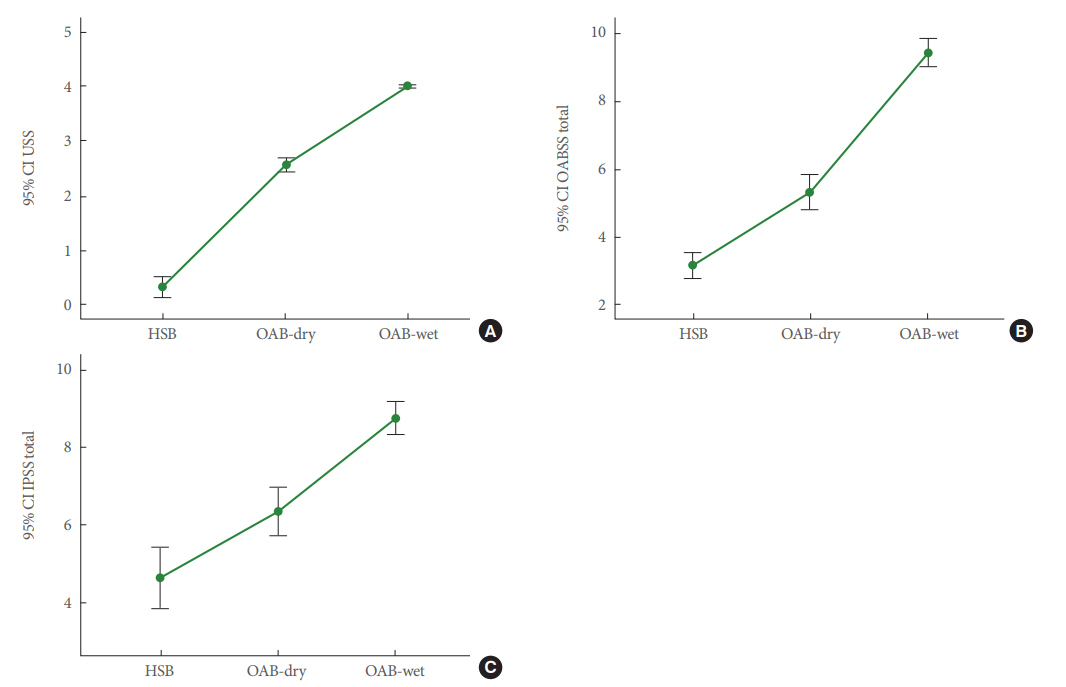
Distribution of OAB subgroup scores according to the USS (A), OABSS (B), and IPSS-S (C) questionnaires. OAB, overactive bladder; USS, Urgency Severity Scale; OABSS, Overactive Bladder Symptom Score; IPSS-S, International Prostate Symptom Score–Storage Subscore; CI, confidence interval; HSB, hypersensitive bladder.
Table 3 shows that the scoring system of each questionnaire had a significant correlation with each OAB subgroup (all P<0.001). The Spearman correlation coefficients (rho) for the USS, OABSS, and IPSS-S were 0.983 (very strong), 0.651 (strong), and 0.428 (moderate), respectively. Fig. 2 shows the areas under the ROC curve for each scoring system and each OAB subgroup. Fig. 2A-C illustrates that the ranking of the AUROC for each OAB subgroup was USS>OABSS>IPSS-S. Table 4 provides the values and comparisons of the AUROC values for each scoring system as related to each OAB subgroup. The AUROC values indicated that the USS was an outstanding discriminative tool for each OAB subgroup (AUROC values of 1.000, 0.953, and 0.994 for HSB, OAB-dry, and OAB-wet, respectively). The OABSS was an outstanding discriminative tool for HSB (0.935), OAB-dry (0.842), and OAB-wet (0.888). The IPSS-S was an excellent discriminative tool for HSB (0.815) and was acceptable for OAB-dry (0.712) and OAB-wet (0.751). All comparisons of the AUROC values of each scoring system for each OAB subgroup showed significant differences (all P<0.001).

Correlation of the OAB subgroups with USS, OABSS, and IPSS-S
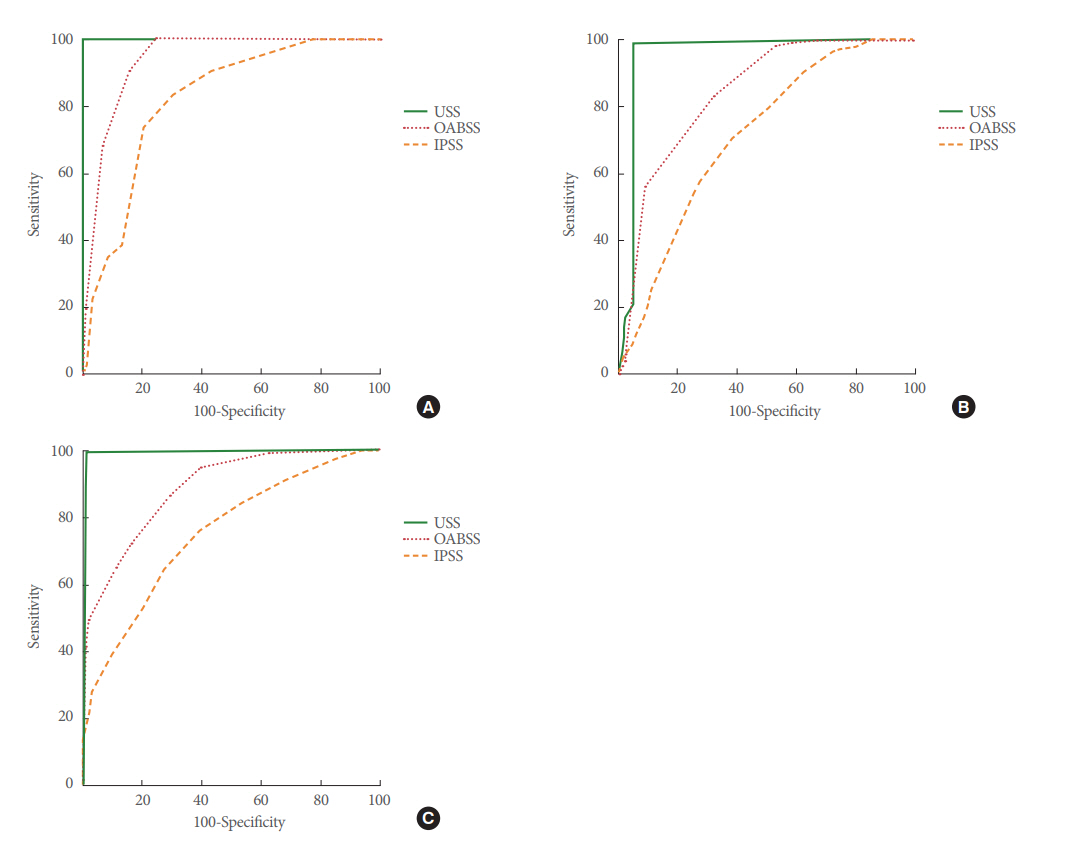
Areas under the receiver operating characteristic (ROC) curves for the USS, OABSS, and IPSS-S by OAB subgroup: (A) HSB, (B) OAB-dry, and (C) OAB-wet. USS, Urgency Severity Scale; OABSS, Overactive Bladder Symptom Score; IPSS-S, International Prostate Symptom Score–Storage Subscore; OAB, overactive bladder; HSB, hypersensitive bladder.
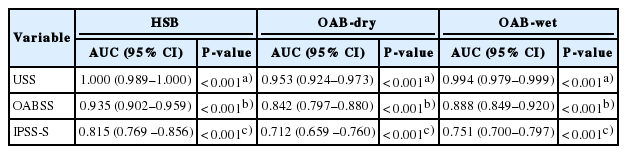
The values and comparisons of the AUC for each questionnaire scoring system by the OAB severity subgroup
The USS, OABSS, and IPSS-S correlated well. The correlation coefficients were 0.628 between the USS and the OABSS-total (P<0.001), 0.682 between the OABSS-total and the IPSS-S total (P<0.001), and 0.340 between the USS and IPSS-S total (P<0.001). Table 5 presents the correlation coefficients between the OAB scoring systems and single items. For the OABSS, OABSS-urgency and OABSS-UUI had a stronger correlation with OABSS-total than OABSS-frequency and OABSS-nocturia did. For the single items, only OABSS-urgency, OABSS-UUI, and IPSS-urgency had a significant correlation with the USS (P<0.001).

Correlation among 3 OAB scoring systems
Table 6 shows the relationships of USS scores with OABSS and IPSS-S scores. Interestingly, among patients with a USS of 0, 1, or 2, the OABSS-total, IPSS-S total, and the single items on the OABSS and IPSS-S did not differ significantly. However, among patients with a USS of 3 or 4, the OABSS-total and IPSStotal were significantly higher than among patients with a USS of less than 3. Moreover, OABSS-frequency, OABSS-nocturia, IPSS-frequency, and IPSS-nocturia did not differ significantly between patients with a USS of 3 or more and those with a USS of less than 3.
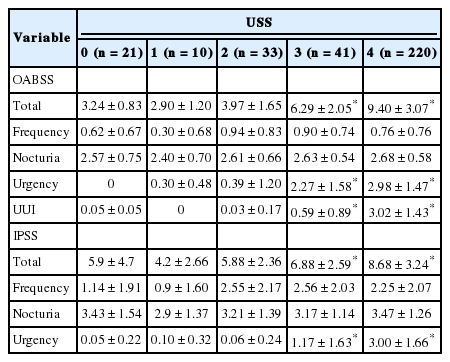
Relationships of USS scores to OABSS and IPSS-S scores
DISCUSSION
The OABSS, IPSS-S, and USS questionnaires correlated well with the OAB subgroups. The ranking of these questionnaires in terms of discriminant ability for characterizing the severity of OAB as HSB, OAB-dry, and OAB-wet was USS>OABSS>IPSSS. One possible reason that the USS outperformed the other questionnaires could have been because the USS has only 1 item for patients to score, whereas the OABSS is the sum of 4 items (frequency, nocturia, urgency, and UUI). The IPSS-S is the sum of 3 items: frequency, nocturia, and urgency. Patients could introduce bias into the assessments of their OAB symptoms.
For wet OAB and dry OAB, patients easily distinguish between episodes of UUI (USS=4), intolerable urgency (USS=3), and tolerable urgency (USS=2). Patients with HSB may report mild urgency (USS=1) or frequency without urgency (USS=0). Because frequency and nocturia are often closely associated with urgency, the scores for frequency and nocturia do not contribute to the severity of OAB. As shown in Table 5, OABSS-total showed the closest correlations with OABSS-urgency and OABSS-UUI, but it was only mildly associated with OABSSfrequency and nocturia. We previously analyzed the correlation between the USS and the OABSS [19]. The main contributions to the OABSS in patients with a low USS were the day- and night-time urination frequencies. The contribution of urgency and UUI became significant in patients with high urgency scores [24]. The findings of the present study concurred with those previous findings. The data imply that frequency and nocturia are common symptoms in all OAB subgroups with varying severity. Only patients with intolerable urgency (USS=3) and urgency with leaking (USS=4) had distinctive OAB symptoms. Therefore, urgency severity (mild, moderate, severe, leakage) alone may be used as a grading system for assessing OAB severity without including scores for frequency and nocturia.
The OABSS is widely used to identify patients with OAB and to evaluate the severity of OAB, as well as treatment outcomes [19,21]. This scoring system is rational and involves all OAB symptoms. The OABSS places different weights on the severity of OAB symptoms of frequency (2 points), nocturia (3 points), urgency (5 points), and UUI (5 points). However, when we correlated the OABSS-total with single items, we found that the correlation was highly significant only for OABSS-urgency (ρ=0.907) and OABSS-UUI (ρ=0.892). OABSS-frequency (ρ=0.300) and OABSS-nocturia (ρ=0.276) were weakly associated with OABSS-total (Table 5). These data indicate that the single item of OABSS-urgency adequately reflected the severity of OAB. Furthermore, because urgency and UUI have a score of 5 points each, the weight of these scores contributes more to the OABSS-total score than items with lesser values.
The IPSS-S system does not have a rating for UUI, so it is difficult to distinguish between wet OAB and dry OAB with intolerable urgency. In addition, the scores for the 3 items (frequency, nocturia, urgency) have equal weighting. Therefore, IPSSfrequency and IPSS-nocturia make a meaningful contribution to the IPSS-total score. As shown in Table 5, the correlation coefficients between the IPSS-S total and its 3 items were similar (ρ=0.629, ρ=0.474, and ρ=0.605, respectively; all P<0.001). However, only the IPSS-urgency and IPSS-S total scores were significantly correlated with the USS (ρ=0.581 and ρ=0.340, respectively; both P<0.001). Moreover, the correlation was more significant for the IPSS-urgency score than for the IPSS-S total score. A similar relationship was found for the correlation between the IPSS-S and OABSS systems. These data confirm the suitability of the definition of OAB recommended by the International Continence Society. OAB should be defined as a symptom syndrome of urinary urgency, with or without urgency incontinence, usually with urinary frequency and nocturia [25]. Urgency is the core symptom of OAB [2,10]. Therefore, the severity of OAB can be rationally classified according to urgency only. For OAB patients, the most bothersome symptom is urgency or UUI when present. The primary limitation of this study is that the relatively high proportion of wet OAB patients (67.7%) may have been a confounding factor.
In conclusion, the simplest questionnaire for the characterization of OAB is the USS (with a scale ranging from 0 to 4), which was found to have the closest correlation with the OAB severity subgroups. The USS alone appears to be adequate for assessing the severity of OAB.
Acknowledgements
Ms. Huei-Ling Tseng for organizing materials to the manuscript. Ms. Chih-Yun Lin for assisting statistical analysis.
Notes
Research Ethics
This study was approved by the Research Ethics Committee of the Buddhist Tzu-Chi General Hospital (TCGH IRB 098-38).
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
·Full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis: HC Kuo
·Study concept and design: HC Kuo
·Acquisition of data: HC Kuo
·Analysis and interpretation of data: HC Kuo, FC Chuang, SM Hsiao
·Drafting of the manuscript: FC Chuang
·Critical revision of the manuscript for important intellectual content: HC Kuo
·Statistical analysis: FC Chuang, SM Hsiao
·Obtained funding: HC Kuo
·Administrative, technical, or material support: FC Chuang, SM Hsiao
·Study supervision: HC Kuo