Alcohol, Smoking, Physical Activity, Protein, and Lower Urinary Tract Symptoms: Prospective Longitudinal Cohort
Article information
Abstract
Purpose:
To evaluate risk factors for deterioration of lower urinary tract symptoms (LUTS) in elderly men in a community-based, prospective longitudinal cohort study.
Methods:
In a suburban area in Korea, 1,514 subjects aged ≥45 years were randomly selected by systematic sampling. A total of 918 elderly subjects were enrolled in this in-depth clinical study in 2004. Of these, 547 participants were followed up for 3 years and the data was analyzed in 2014. Standard questionnaires were administered face-to-face by trained interviewers. After excluding women, 224 male participants with complete data including transrectal ultrasonography were included in the final analysis. LUTS were diagnosed using the International Prostate Symptom Score (IPSS) questionnaire. Symptom deterioration was defined as a score of ≥8 points during the 3-year follow-up period.
Results:
LUTS prevalence increased to 13.1% and the mean IPSS increased by 2.6 points during the 3-year period. After adjusting for confounders, a smoking history of ≥50 pack-years was an independent risk factor for deterioration of LUTS and storage subsymptoms compared with no history of smoking (3.1 and 5.1 odds, respectively). Physical activity had a protective effect on voiding subsymptoms. However, high protein diet and alcohol intake were not associated with LUTS deterioration.
Conclusions:
The LUTS prevalence among elderly men living in a suburban area increased to 13.1% and the IPSS increased by 2.6 points during the 3-year period. A history of heavy smoking, low physical activity, and high protein intake were associated with LUTS deterioration. However, there was no significant association between alcohol intake and LUTS deterioration.
INTRODUCTION
Elderly men commonly experience lower urinary tract symptoms (LUTS), regardless of their region of origin and ethnicity [1]. These symptoms can be bothersome and can greatly hinder the quality of life of affected individuals [2]. In the United States, more than 4.5 million patients presented to physicians on an outpatient basis with LUTS as their major complaint, and the direct cost of LUTS/benign prostatic hyperplasia (BPH) treatment was approximately 1.1 billion United States dollars in 2000 [3]. In elderly men, LUTS/BPH is a progressive condition that can cause serious complications such as acute urinary retention [4].
Recent epidemiological and clinical studies have suggested an association between LUTS and modifiable risk factors. Several studies suggested that diet, physical activity, alcohol, and smoking were modifiable factors that can either increase or decrease the risk of LUTS progression [5-10]. However, the etiology and natural history of LUTS are not well understood.
Increased physical activity and vitamin C intake have been linked to a decreased risk of LUTS [5,10-13]. On the other hand, protein and sodium intake were associated with an increased risk [11,14]. The data with respect to the association between LUTS and alcohol or smoking are conflicting [7,9,10,15]. Although several cross-sectional studies have analyzed each factor individually, few studies have performed multivariable analyses that considered all modifiable lifestyle factors. In addition, very few longitudinal studies have been conducted.
Therefore, we aimed to evaluate risk factors for the deterioration of LUTS in elderly men in a community-based, prospective longitudinal cohort study.
MATERIALS AND METHODS
Study Design and Subjects
The Hallym Aging Study was a prospective cohort study that investigated the quality of life and health of elderly community residents in the suburban city of Chuncheon, Korea. Based on a population-based epidemiologic survey of the elderly in 2003, an in-depth clinical study was initiated in 2004. Follow-up exams at 3-year intervals were performed in 2007 and 2010. The data for this study were analyzed in 2014. The study protocols and informed consent procedures were approved by the Ethics Committee of Hallym University and Dongtan Sacred Heart Hospital (DTF 06-001-2014-309). This study was performed in strict accordance with the ethical guidelines of the Declaration of Helsinki. Written informed consent was obtained from all study participants at the time of their enrollment in the study.
The city was divided into 1,408 areas based on the Korean National Census conducted in 2000, and 200 enumeration districts were randomly selected to proportionately represent residential areas. After allocating a number of individuals based on the ratio of those aged ≥45 years in each area, subjects were selected through systematic sampling.
Individuals aged ≥45 years who resided within the limits of the survey area for at least 6 months before the study began and had sufficient mental and physical capacity to participate were eligible for the study. The primary survey panel in 2003 included 1,510 participants who responded to the survey (451 people aged 45–64 years and 1,059 people aged ≥65 years) who were enrolled as subjects in the first in-depth clinical study.
A total of 918 individuals agreed to participate in the indepth clinical study and completed personal interviews at baseline in 2004. A total of 547 subjects agreed to participate in the follow-up examination in 2007. Finally, 224 subjects who underwent transrectal ultrasonography of the prostate were included in the final analysis (Fig. 1).
Patient disposition flow chart.
Data Collection
This investigation consisted of questionnaires, anthropometric measurements, and laboratory tests. Standard questionnaires were personally administered by trained interviewers. The questionnaire requested sociodemographic information on age, educational attainment, marital status, household income, occupation, and comorbidities. Anthropometric measurements and laboratory tests were performed by a hospital clinical team. All measurements were performed in accordance with prespecified standard protocols and were monitored by regular quality control checks. Anthropometric measurements were performed with subjects wearing lightweight clothing and no shoes. Height and weight were obtained using an automatic height/weight measurement system (DS-102, JENIX, Seoul, Korea), and body mass index (BMI) was determined using the following formula: (weight/height2; kg/m2). Systolic and diastolic blood pressure measurements were taken twice by a skillful family medicine resident after the subject remained at rest for >10 minutes. The mean values were used for the purpose of this study. Blood samples were drawn from the antecubital vein in the morning after an overnight fast of >10 hours.
LUTS and Deterioration of LUTS
The presence and degree of LUTS were evaluated using the International Prostate Symptom Score (IPSS) questionnaire, which consisted of seven domains including incomplete emptying, frequency, intermittency, urgency, weak stream, straining, and nocturia. The IPSS was divided into subsymptoms of voiding and storage. The voiding subscore was the sum of the IPSS domains of incomplete emptying, intermittency, weak stream, and straining. The storage subscore was the sum of the domains of frequency, urgency, and nocturia. Individuals were diagnosed with LUTS if the total IPSS was ≥8 points at baseline, and the deterioration of LUTS was defined as an increase of ≥8 points in the IPSS during the 3-year follow-up period [16]. An increase of ≥5 points in the voiding subscore was considered deterioration of voiding subsymptoms during the 3-year follow-up period. Deterioration of storage subsymptoms was defined as an increase of ≥4 points in the IPSS storage subscore during the follow-up period [13].
Dietary Intake
Dietary intake was assessed using the semi-quantitative food frequency questionnaire (SQ-FFQ), which included 98 commonly consumed food items selected from the results of the Korean Health and Nutritional Survey in 1998 [17]. The 98 food items that were included in the questionnaire are as follows: 12 in the cereal group, 5 in the noodle and bread group, 4 in the starch group, 13 in the meat group, 2 in the egg group, 3 in the milk group, 6 in the soybean and soybean-derived products group, 10 in the fish and shellfish group, 15 in the vegetable group, 2 in the seaweed group, 12 in the fruit group, 5 in the beverage group, 2 in the tea group, 3 in the snack group, and 4 in the alcohol group. Each subject was interviewed using the SQ-FFQ and the 24-hour recall method. The nutrient intake of each food item was converted based on the weight derived from the consumption frequency and the portion size. The daily nutrient intake of each individual was the sum of the nutrient intake of each food item. The intake of dietary vitamin C from foods and beverages was divided based on 100 mg/day, which is the amount contained in a cup of orange juice [18]. A highsodium diet was defined as a dietary sodium intake of ≥6 g per day [19]. A low-protein diet was defined as a dietary protein intake of <14.6% of the daily calorie requirement [20].
Smoking
Using a questionnaire, smoking status was categorized as never, former (≥100 cigarettes smoked in a lifetime and >1 year of not smoking), or current smoker. For former and current smokers, data on the duration and the amount of past and current use of cigarettes, age at initiation, and date and year when smoking stopped were obtained. Data on the number of cigarettes smoked per day over the previous 12 months were collected. This study also calculated pack-years (PY) of smoking based on smoking history; a PY was defined as 20 cigarettes per day for 1 year. A history of heavy smoking was defined as ≥50 PY of smoking in a lifetime [5].
Alcohol
Subjects were asked to report their alcohol intake on a weekly basis. Current alcohol drinkers were asked about the frequency and amount of consumption per occasion of 5 alcoholic beverages: Makgeolli (Korean raw rice wine), Soju (Korean distilled spirits), beer, whiskey, and wine. For an estimation of the total alcohol intake in grams per day, the number of grams per drink multiplied one standard drink of a specific type of alcoholic beverage. One standard drink was defined as one unit of alcohol, which was equal to 8 to 13 g of alcohol. For beer, one standard drink was equal to 1 can of beer (330 mL, 5%, 13.2 g of alcohol), which was equivalent to 1 glass of wine (125 mL, 13%, 13 g of alcohol) or Makgeolli (250 mL, 6%, 25 g of alcohol), as well as 1 shot of Soju (50 mL, 19%, 8 g of alcohol) or whiskey (35 mL, 43%, 12 g of alcohol) [21]. Daily ethanol intake was calculated from participant responses regarding their daily frequency of alcohol intake in each beverage and the number of days per week that they consumed alcohol. A heavy drinker was defined as an individual who consumed ≥40 g/day of alcohol (approximately 3 cans/day) [5,22].
Physical Activity
The intensity of physical activity in the previous year was ascertained during the interview. The Korean version of the Minnesota Leisure Time Physical Activity Questionnaire was used to measure physical activity [23]. Participants were asked about the type, frequency, and average duration of 63 activities divided into 9 general categories. The participants were asked to estimate the average number of minutes per week each activity was performed during each season. The total energy expenditure per week was calculated using the activity metabolic index, which allowed measurement of the number of calories that were burned using the metabolic equivalent for each task [24]. Lack of physical activity was defined as <140 kcal consumption per day [25].
Statistical Analyses
For descriptive statistics such as baseline characteristics, categorical data were expressed as numbers and percentages, and continuous data as the mean±standard deviation. In comparative analyses, categorical variables were compared for subjects with or without deterioration of LUTS using chi-square or Spearman tests, and continuous variables were compared using Student t or Mann-Whitney U tests. All lifestyle variables were categorized using reference levels obtained from previous studies. Longitudinal analyses were conducted with paired t or Wilcoxon signed rank tests and repeated analysis of variance using baseline lifestyle factors and the outcome of LUTS deterioration between baseline and follow-up. Logistic regression was used to calculate the age-adjusted odds ratio (OR) and 95% confidence interval (CI) for the deterioration of LUTS in the longitudinal analysis. Separate analyses were conducted for the voiding and storage symptom subtypes of LUTS. In addition, each individual item of IPSS was analyzed. Multivariable models were derived by including all variables associated with outcome (P <0.20) in an age-adjusted model and retained potential confounders judging from the investigator. A two-sided P≤0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
The mean age of the participants was 68.7±7.6 years at the time of study initiation. Of the participants, 54 (24.1%) were current smokers, and 65 (29.0%) were heavy drinkers (consumed ≥3 cans of beer per day). With respect to leisure time and physical activity, participants consumed an average of 146.9±13.2 kcal daily. The average daily protein intake was 59.5±1.5 g and the average volume of the prostate was 31.3±10.8 mL (Table 1).

Baseline characteristics of study participants and comparison analyses according to deterioration of LUTS during 3 years
Of the 224 participants, 124 (55.4%) had moderate or severe LUTS at baseline, which increased to 153 (68.3%) after the 3-year follow-up period and corresponded to an increase of 13.1% in the prevalence of LUTS during the follow-up period, and 4.43% per year (Fig. 2A). The average of the total IPSS increased by 2.56±8.86 points, from 10.73±8.89 to 13.29±9.11 (P <0.001). The average voiding and storage subscores increased by 1.27 ±6.38 points, from 6.52 ±6.21 to 7.79 ±5.78 (P <0.001), and by 1.29±3.66, from 4.21±3.91 to 5.50±3.94 (P <0.001), respectively, over 3 years (Fig. 2B).

Deterioration of lower urinary tract symptoms (LUTS) during the 3-year follow-up period. (A) Changes in the prevalence of moderate to severe LUTS in elderly men during the 3-year follow-up period; (B) changes in the International Prostate Symptom Score (IPSS) total score, voiding and storage symptoms, and the quality of life (QoL) subscore in elderly men during the 3-year follow-up period. *P≤0.05.
There was no difference in the deterioration of LUTS between participants who consumed an average of ≥40 g of alcohol daily and those who consumed less (Fig. 3A). Heavy smokers (smoked ≥50 PY of cigarettes in a lifetime) showed a significant deterioration of storage subsymptoms (≥50 PY vs. <50 PY, 2.47±4.29 vs. 0.98±3.43, P=0.033), and there was a marginal statistical association with a greater deterioration of the total IPSS (≥50 PY vs. <50 PY, 4.60 ±9.99 vs. 2.04 ±8.49, P=0.080) (Fig. 3B). In addition, heavy smokers had significant deterioration in the nocturia subdomain of the IPSS (≥50 PY vs. <50 PY, 1.25±0.18 vs. 1.01±0.76, P=0.038). Participants with an average of <140 kcal of daily energy consumption during leisure time and physical activity experienced more severe exacerbation of voiding subsymptoms during the 3-year follow-up period (<140 kcal vs. ≥140 kcal, 2.03±6.29 vs. 0.21±6.63, P=0.046) (Fig. 3C). Participants who had a protein intake that was <14.6% of the daily calorie requirement presented with less deterioration of the total IPSS and voiding subsymptoms (<14.6% vs. ≥14.6%; IPSS: 1.88±9.58 vs. 4.83±8.48, P=0.027; voiding subscore: 0.88 ±6.13 vs. 2.78 ±6.71, P =0.044) (Fig. 3D). The deterioration of voiding subsymptoms was more severe if vitamin C intake was <100 mg/day (<100 mg vs. ≥100 mg, 2.32±6.98 vs. 0.56±5.73, P=0.047) (Fig. 3E). If the daily intake of sodium was ≥6 g, the total IPSS and storage subsymptoms worsened significantly (≥6 g vs. <6 g; IPSS: 4.10±8.85 vs. 1.44±8.65, P=0.031; storage subscore: 2.00±3.62 vs. 0.73±3.66, P=0.014) (Fig. 3F).
Deterioration of lower urinary tract symptoms (LUTS) and subsymptoms during the 3-year follow-up period in accordance with modifiable lifestyle factors. (A) Alcohol consumption: <40 mg/day vs. ≥40 mg/day; (B) smoking status: <50 pack-years (PY) vs. ≥50 PY; (C) leisure time physical activity: ≥140 kcal/day vs. <140 kcal/day; (D) protein intake: <14.6% vs. ≥14.6%; (E) vitamin C intake: ≥100 mg/day vs. <100 mg/day; (F) sodium intake: <6 g/day vs. ≥6 g/day. IPSS, International Prostate Symptom Score; QoL, quality of life. *≤0.05. † P≤0.10.
The results of the multivariate analysis using logistic regression showed that a history of heavy smoking significantly exacerbated the total IPSS (P=0.028; OR, 3.07; 95% CI, 1.13–8.36) and storage subsymptoms (P <0.001; OR, 5.13; 95% CI, 2.25–11.67). Lack of physical activity had an independently significant adverse effect on the deterioration of voiding subsymptoms (P=0.039; OR, 2.25; 95% CI, 1.04–4.87). Nocturia was significantly worse in heavy smokers (P =0.005; OR, 6.61; 95% CI, 1.75–25.00). However, a high-protein diet, vitamin C intake, and sodium consumption did not significantly affect the deterioration of LUTS after adjustment for potential confounding factors such as age, BMI, underlying diseases, and prostate volume (Table 2).
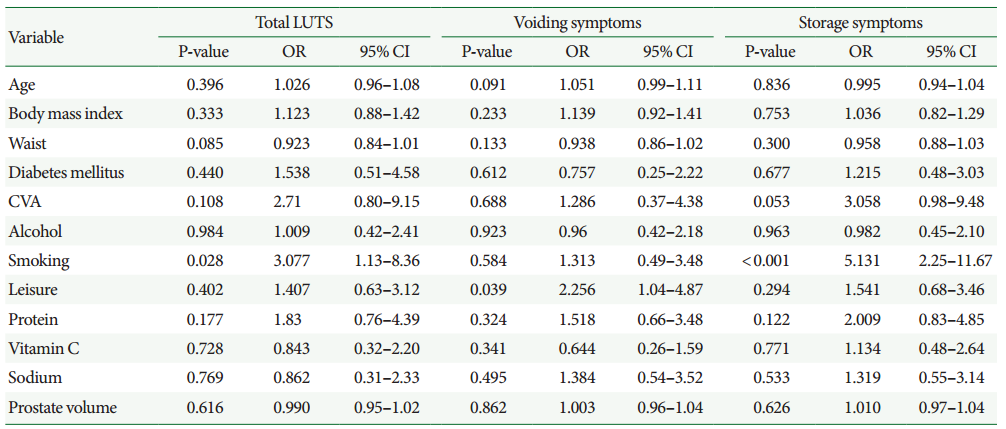
Multivariable logistic regression analysis of risk factors for deterioration of LUTS in elderly men
DISCUSSION
We analyzed modifiable lifestyle factors that could affect the deterioration of LUTS in a prospective longitudinal cohort study. It was determined that the deterioration of LUTS, particularly of storage symptoms, was severely exacerbated in heavy smokers. Exercise was found to be a protective factor for voiding symptoms. The total energy intake-adjusted protein consumption was associated with storage symptoms. Notably, alcohol consumption was not directly associated with the development of LUTS in elderly men. The findings of this study are expected to be widely used as basic data regarding prevention of the deterioration of LUTS.
In this study, the prevalence of LUTS was 55.4% among Korean men with a mean age of 68.7 years. After the 3-year follow-up period, the prevalence of LUTS increased by 4.43% per year to 68.3%. During the 3-year follow-up period, the total IPSS of the participants increased by 2.6 points on average, from 10.7 to 13.2 points. A mean increase of 1.27 and 1.29 points was observed in the voiding and storage subscores, respectively. Parsons [8] reported that 29% of men without LUTS at baseline developed moderate to severe symptoms within 2 years of follow-up. Similarly, 21% of Japanese, 26% of African American, and 20% of Austrian men without symptoms or with very mild symptoms at baseline reported clinically significant LUTS after 3, 4, and 5 years of follow-up, respectively. Although prostate volume was not associated directly with symptom severity, it was reported to increase with a 2.0%–2.5% growth rate per year among elderly men [7].
In this study, heavy smoking was found to increase the risk of LUTS exacerbation, and mainly affected storage symptoms. Participants who smoked ≥50 PY in a lifetime had 5.1 times greater probability of severe deterioration of storage symptoms. In a recent study, Tahtinen et al. [26] also reported that heavy smoking was associated with urgency and frequency symptoms. Nicotine increased sympathetic nervous system activity and could contribute to storage symptoms by increasing the tone of the bladder smooth muscle [5,27]. Furthermore, smoking could cause hormonal and nutrient imbalances affecting the bladder as well as collagen synthesis [10]. It has also been reported to affect bladder wall strength and detrusor instability [28].
There was no direct association between alcohol consumption and LUTS. Additionally, it was found that heavy drinking (>40 g/day) was not a risk factor for exacerbation of LUTS. This result is consistent with those of a recent meta-analysis, which reported that alcohol consumption was not a significant risk factor for LUTS [9]. Moderate alcohol intake has been linked to a decreased risk of coronary artery disease, and this beneficial effect on the cardiovascular system may have also had a protective effect on BPH progression [9,29]. Interestingly, the protective effect did not extend to LUTS. Unlike BPH, LUTS involves both prostate- and bladder-related factors. The diuretic and other systemic effects of alcohol such as changes in insulin sensitivity and hormone levels are considered to directly or indirectly affect bladder function [5].
Participants who were physically active during leisure time were less likely to experience a deterioration of voiding symptoms. Cardiovascular disease and metabolic syndromes may increase the risk of LUTS, which is independent of prostate enlargement [30]. However, physical activity was found to reduce the risk of LUTS, and this outcome was considered to result from improvements in cardiovascular health, promotion of weight loss, enhancement of vascular flow, and normalization of serum lipid and lipoprotein concentrations [11]. Physical activity was also associated with the improvement of insulin sensitivity and changes in sympathetic nervous system activity [5]. It is possible that physical activity directly influences prostate growth pathways through the alteration of hormone levels [11].
The main limitation of this study was that a large number of participants quit (nearly a third of the total number of participants originally enrolled). This study was conducted in a geographically limited area (the suburban city of Chuncheon) where individuals had poor accessibility to the hospital. In addition, it is possible that there was selection bias given the nature of the study design and the high proportion of women among the elderly population. To minimize the effects of this potential weakness, participants were randomly selected through systematic sampling of 200 areas. In addition, considerable efforts were made to reduce the unavoidable problem of community-based longitudinal studies by contacting participants by telephone and/or mail. Another potential limitation was that the deterioration of LUTS was evaluated only by using the IPSS during the 3-year follow-up period. LUTS have been shown to be dynamic, with progression or remission of symptoms over time. Thus, some participants may have been misclassified as symptom-free at follow-up. However, the standard questionnaires were administered personally by well-trained, seasoned interviewers, i.e., data were not collected through self-reporting; this can be considered a strength of this study. Another weakness of this study was the relatively small sample size. Finally, as these results were obtained from a suburban population of elderly men in Korea, they may not be generalizable to other populations.
In this study, the prevalence of LUTS in elderly men living in a suburban area in Korea increased by 13.1%, from 55.4% to 68.3%, during the 3 years of follow-up. The IPSS increased by 2.6 points on average, from 10.7 to 13.2. A history of heavy smoking was identified as risk factors for the deterioration of LUTS that mainly affected storage symptoms. Participants who performed less physical activity were more susceptible to worsening of voiding symptoms during the 3-year follow-up period. There was no significant association between alcohol or protein intake and the deterioration of LUTS. Based on these findings, it may be possible to prevent the deterioration of LUTS by reducing smoking and increasing physical activity among individuals.
Notes
Fund Support
This study was supported by the Hallym University Research Fund 2014 (HURF-2014-57).
Research Ethics
The study protocols and informed consent procedures were approved by the Ethics Committee of Hallym University and Dongtan Sacred Heart Hospital (DTF 06-001-2014-309). This study was performed in strict accordance with the ethical guidelines of the Declaration of Helsinki.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.