Atrophy of the Tongue as the Presenting Feature of Metastatic Prostate Cancer
Article information
Abstract
Prostate cancer is the most frequently diagnosed solid organ cancer in men and is the second leading cause of cancer-related deaths in men in the United Kingdom. Commonly, it metastasizes to bones and lymph nodes, however, in advanced hormonerefractory disease it may involve the skull base leading to associated cranial nerve palsies. Cranial nerve palsy as the presenting feature of advanced hormone-sensitive prostate cancer is extremely rare. To the best of our knowledge, we report the first case of solitary hypoglossal nerve palsy as the presenting feature of advanced prostate cancer. Neurologists, neurosurgeons and otolaryngologists may be the first clinicians to see such a patient; therefore, prostate cancer should be amongst the differential diagnoses considered in middle-aged and elderly men presenting with a cranial neuropathy and evidence of skull metastasis.
Prostate cancer commonly metastasizes to skeletal bones and lymph nodes. The vast majority of skeletal bone metastases involve the axial spine, pelvis and femora [1]. Uncommonly, the skull base may be involved, almost exclusively; in prostate cancer this is associated with hormone-refractory cancer. Skull base involvement may lead to cranial neuropathies [2,3]. Cranial neuropathy as the presenting feature is extremely rare [4], and although, there is one reported case of hypoglossal nerve involvement as the presenting feature, this was associated with involvement of multiple cranial nerves at the time of presentation. To the best of our knowledge, we report the first case of solitary hypoglossal nerve palsy as the presenting feature of advanced prostate cancer.
CASE REPORT
A 74 year old male presented to his family physician with intermittent right sided headaches of 2 months duration. There was no history of trauma, migraine and no associated neck pain. Otherwise, his general health was very good. Clinical examination was unremarkable, therefore, no further investigations were instigated and the patient was discharged with simple analgesia.
Four months later, he returned to his family physician with worsening symptoms, namely, the headaches became more intense, persistent and were associated with slurred speech. Clinical examination revealed atrophy of the right side of the tongue and deviation to the right on protrusion - right hypoglossal nerve palsy (Fig. 1) but no other neurological abnormalities were noted. He was referred to the local neurologist for further management. His baseline blood tests which included a whole blood count, urea and electrolytes, serum calcium and glucose were all normal. A computed tomography of the brain showed skull base sclerotic metastases, subsequently, a magnetic resonance imaging of the brain revealed a focal abnormality of the right petrous bone with involvement of the hypoglossal nerve (Fig. 2). Bone metastases are commonly associated with thyroid, lung, breast, prostate and renal cancer, prostate cancer differs from the others by nature of its' sclerotic bone metastases. Therefore, in addition to the chest X-ray, ultra sound scan of the renal tract, a serum prostate specific antigen (PSA) was requested, this was found to be elevated at 101 ng/mL. He was then referred to a urologist with suspected prostate cancer.

Patient with a right sided hypoglossal nerve palsy.
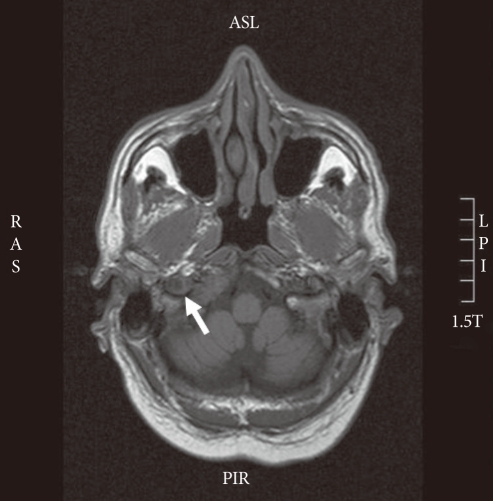
Magnetic resonance imaging shows an abnormality of the right petrous bone and hypoglossal nerve.
He denied suffering from lower urinary tract symptoms and there was no history of back pain. Clinical examination of the prostate gland revealed a T3 cancer. Subsequently, prostate gland biopsies confirmed a well-differentiated adenocarcinoma, Gleason score 3+3=6. A bone scan revealed widespread bony metastases.
Although, there has been no recovery of the hypoglossal nerve palsy following a bi-lateral scrotal orchidectomy, his recent PSA level remains low at 3.2 ng/mL. At 32 months of follow-up he has not required second line treatment or palliative radiotherapy.
DISCUSSION
Skull base metastatic cancer is often silent; however, as the disease advances it commonly results in cranial nerve palsies. A combination of computed tomography and magnetic resonance imaging of the head is used to diagnose skull base metastases. Although rare, cranial nerve palsies are associated with advanced prostate, breast, lymphoma and lung cancers [5]. Collet-Sicard syndrome is caused by a lesion that involves the lower 4 cranial nerves. It results in the paralysis of vocal cords, palate, trapezius and sternocleidomastoid muscles. Clinically, it results in anaesthesia of the larynx, pharynx and soft palate [6]. As described in our patient, unilateral occipital headache with ipsilateral hypoglossal nerve palsy is termed occipital-condyle syndrome [7]. Although, sclerotic bone metastases are commonly associated with prostate cancer, other cancers with bone metastases must be excluded; such as thyroid, lung, breast and renal cancer. Skull base involvement of metastatic prostate cancer is almost invariably associated with known hormone-refractory disease. Cranial neuropathy as the presenting feature is extremely rare [4], and although, there is one reported case of hypoglossal nerve involvement as the presenting feature, this was associated with involvement of multiple cranial nerves at the time of presentation. To the best of our knowledge, we report the first case of solitary hypoglossal nerve palsy as the presenting feature of advanced prostate cancer. Neurologists, neurosurgeons and otolaryngologists may be the first clinicians to see such a patient; therefore, prostate cancer should be amongst the differential diagnoses considered in middle-aged and elderly men presenting with a cranial neuropathy and evidence of skull metastasis. Furthermore, if a PSA test is elevated then the patient should be referred to the urologist.
Notes
No potential conflict of interest relevant to this article was reported.