Condyloma acuminata is often reported to develop in adult anal or genital regions. However, it rarely occurs in the female urethra and seldom causes bladder outlet obstruction (BOO). We report a case of urethral condyloma in a woman who presented BOO-related voiding symptoms.
CASE REPORT
A 39-year-old woman presented to our hospital complaining of frequency, urgency, and sensation of incomplete bladder emptying. Urinalysis revealed no microscopic hematuria or pyuria, and her urine culture remained sterile. An uroflowmetry was performed, and the free maximum flow rate (Qmax) was low at 14 mL/sec, with voided volume at 218 mL, and postvoid residual urine volume (PVR) at 25 mL. She was administered an alpha blocker for two weeks, but there was no symptom improvement. A follow-up uroflowmetry showed an even lower Qmax at 8 mL/sec, with voided volume at 206 mL, and PVR at 45 mL. To rule out any anatomical obstructing lesions, a physical examination was performed, and multiple small papillary masses were noted around the external urethral meatus (Fig. 1).
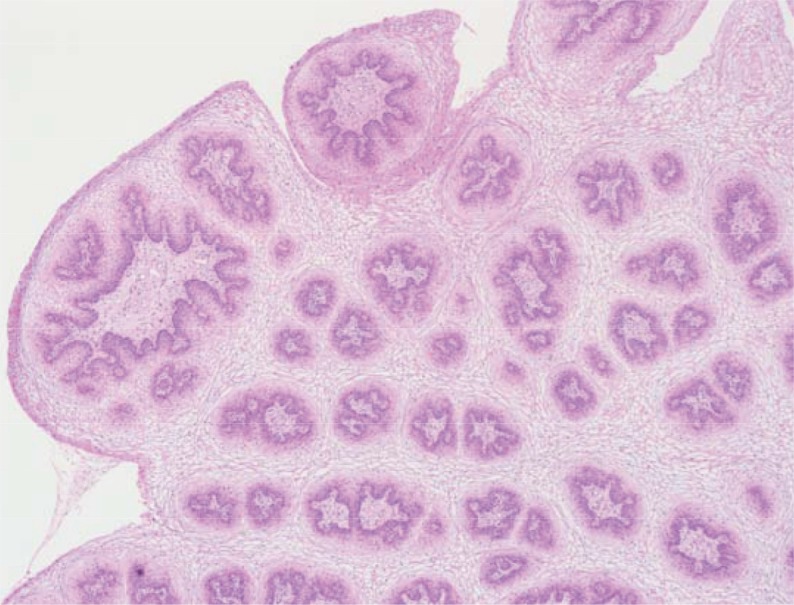
The rapid plasma reagin card test and Treponema pallidum hemagglutination test results were negative. Cystourethroscopy demonstrated nonspecific findings in the urethra and bladder. An urodynamic study revealed a detrusor pressure at maximum flow rate (PdetQmax) at 25 cm H2O with Qmax at 14 mL/sec, indicating BOO. The masses were surgically excised, and primary repair was performed. Histopathological examination indicated condyloma acuminata with papillomatosis, acanthosis, parakeratosis, and hyperkeratosis (Fig. 2).
Excision of the masses resulted in near complete resolution of her symptoms. No obvious recurrence of condyloma acuminata has been observed for 6 months after the surgery. One month after the surgical excision, a follow-up uroflowmetry showed an improved Qmax, voided volume, and PVR at 17 mL/sec, 229 mL, and 10 mL, respectively.
DISCUSSION
There are no absolute criteria to define female BOO so far, but several reports have indicated that a Qmax less than 15 mL/sec combined with a PdetQmax greater than 20 cm H2O in a pressure-flow study is associated with obstructive symptoms [1]. In women, BOO can present with various types of symptoms. Typical complaints of slow urinary flow and difficult emptying are highly indicative of BOO. Many other voiding problems such as irritative voiding complaints following BOO make it more difficult to diagnose [2]. This reinforces the need for a thorough investigation in women with BOO, including careful history taking and physical examination, with other appropriate imaging, functional studies.
The causes of BOO can be classified as anatomical or functional [3]. In women, anatomical causes of BOO include extrinsic compression by Skene's gland cysts, diverticulum, and Gartner's duct remnants. Moreover, genitourinary malignancy including urethral cancer and numerous gynecologic cancers can induce urinary obstruction and should always be considered in the diagnostic algorithm.
Condyloma acuminata is a common sexually transmitted disease caused by the human papillomavirus infection [4]. It is mostly found in young adults between 17-33 years of age, and the incubation period varies from weeks to months [5]. Associated symptoms such as split stream, dysuria, urethral bleeding, and infection are not so common. Condyloma acuminata consists of soft, papillary growths occurring singly or in clusters, and presents in moist areas such as the genitalia, rectum, and urethra. Urethral condyloma is relatively uncommon in both men and women. Even more uncommon is the occurrence of BOO due to urethral condyloma. Various treatment methods have been used, including 5-fluorouracil, interferon, electrocoagulation, cryotherapy, photodynamic therapy, carbon dioxide laser, and local excision. Condyloma treated with electrocoagulation or laser evaporation has high recurrence rates, and urethral stenosis, erosion, and adhesion can occur as complications [6].
In conclusion, female urethral condyloma is a rare entity, and it rarely causes BOO. It should be considered as a differential diagnosis in women presenting with obstructive voiding symptoms associated with a urethral mass. The present case emphasizes that a thorough physical examination should be performed in young women with signs of BOO. In women, excision of urethral condylomas causing obstruction can be an effective treatment with early recovery of voiding function.