The Role of Robotics in Meeting Institutional Goals: A Unified Strategy to Facilitate Program Excellence
Article information

Abstract
Purpose
The rapid expansion of robotic surgical equipment necessitates a review of the needs and challenges faced by hospitals introducing robots for the first time to compete with experienced institutions. The aim of this study was to analyze the impact of robotic surgery on our hospital compared to open and laparoscopic surgery, examine internal transformations, and assess regional, domestic, and international implications.
Methods
A retrospective review was conducted of electronic medical records (EMRs) from 2019 to 2022 at Inha University Hospital, including patients who underwent common robotic procedures and equivalent open and laparoscopic operations. The study investigated clinical and operational performance changes in the hospital after the introduction of robotic technology. It also evaluated the operational effectiveness of robot implementation in local, national, and international contexts. To facilitate comparison with other hospitals, the data were transmitted to Intuitive Surgical, Inc. for analysis. The study was conducted in compliance with domestic personal information regulations and received approval from our Institutional Review Board.
Results
We analyzed EMR data from 3,147 patients who underwent surgical treatment. Over a period of 3.5 years, the adoption of robotic technology in a hospital setting significantly enhanced the technical skills of all professors involved. The introduction of robotic systems led to increased patient utilization of conventional surgical techniques, as well as a rise in the number of patients choosing robotic surgery. This collective trend contributed to an overall increase in patient numbers. This favorable evaluation of the operational effectiveness of our hospital’s robot implementation in the context of local, national, and global factors is expected to positively influence policy changes.
Conclusions
Stakeholders should embrace data science and evidence-based techniques to generate valuable insights from objective data, assess the health of robot-assisted surgery programs, and identify opportunities for improvement and excellence.
INTRODUCTION
Robotic-assisted surgery is increasingly popular worldwide, as the capability for minimally invasive surgery is essential in contemporary healthcare [1, 2]. The trend toward more widespread use of robotic surgery is driven by its potential benefits, including an ergonomic design, enhanced surgical precision, improved tissue visualization, reduced need for surgical assistance, and better training and workflow procedures [3-6]. To date, over 14.8 million surgical procedures have utilized da Vinci robots (Intuitive Surgical, Inc., Sunnyvale, CA, USA) globally, and during the past 5 years, including the coronavirus disease 2019 epidemic, the average annual growth rate of procedures was 17%, with more than 9,400 surgical platforms recently deployed worldwide [7, 8]. This reflects a significant and rapid increase in the number of hospitals adopting robotic systems for the first time. In South Korea, 160 robot systems have been installed in 96 hospitals as of 2023, with 40 hospitals introduced in the last 5 years, representing 41.7% of all hospitals [8]. This swift expansion is likely to lead to performance disparities among hospitals based on their experience since the initial introduction of robots, necessitating efforts to minimize these differences. In this era of rapid growth in robotic surgical equipment, it is crucial to assess the needs of hospitals implementing robots for the first time and to address the challenges they face to keep pace with more experienced institutions.
There is a strong business rationale for scientific research on implementation. As healthcare systems become increasingly dynamic and resource-constrained [9], evidence-based techniques are essential for ensuring that hospital investments maximize healthcare value while also improving patient health [10, 11]. The evidence for robotic surgery involves analyzing operations performed at these hospitals. This analysis requires not only an internal review within the hospital but also a comparison with hospitals equipped with robots in the surrounding area, domestically, and internationally [12]. Comparisons of this type are crucial for assessing the hospital’s current status and informing future robot-related policy decisions. Following the successful introduction of the da Vinci system at our hospital (Inha University Hospital) on December 24, 2018, we recognized the importance of gathering evidence from robot-related procedures performed at our hospital over a 3-year period. Our hospital’s strategic planning division conducted an analysis, but the findings did not meet our expectations. At the time, we were unaware that such an analysis program existed, so we reached out to Intuitive, a global robot manufacturing company, for information. After learning about Intuitive’s Custom Hospital Analytic (CHA) program, we decided to participate. Since no such program existed in our country at that time, we faced many challenges. However, this analysis, which we could not undertake on our own, would allow us to evaluate our hospital’s current and future direction by comparing the performance of our robotic surgery center with that of other hospitals performing robotic surgery locally and globally.
The program, which is operated by former hospital operators and analysts now employed at Intuitive, has been designed to assist hospitals in validating their robotic programs and planning for excellence. A CHA report provides a visualization of the current state of the robotic surgery program using the da Vinci system, based on clinical, financial, and operational metrics. This supports hospitals in making informed decisions regarding clinical standards, financial feasibility, and program optimization. The service is governed by an analytics agreement to ensure privacy protection and undergoes regular audits to maintain HIPAA (Health Insurance Portability and Accountability Act) compliance. In the United States, 742 hospitals have engaged with CHA in more than 3,650 instances. Approximately 60% of hospitals with a CHA agreement update their original data submissions to monitor and evaluate changes in their da Vinci program. The growing demand for this service has contributed to the creation of a database containing over 4.8 million surgical encounters to date.
The aim of this study was to assess the impacts of robotic surgery at Inha University Hospital compared to 2 conventional surgical techniques —open surgery and laparoscopic surgery—from clinical and surgical perspectives. The second objective was to analyze the internal transformations within the hospital following the implementation of robotic systems, and to assess the regional, domestic, and international implications of these changes. Additionally, the study sought to identify and specify areas for improvement to achieve global excellence for the hospital in the future.
MATERIALS AND METHODS
We conducted a retrospective review of electronic medical records (EMRs) for all consecutive patients who underwent one of the following surgical operations at Inha University Hospital in Incheon, a single academic institution, from January 1, 2019 to June 30, 2022. The inclusion criteria included a history of the 5 most common robotic procedures during the period, as well as the equivalent open and laparoscopic surgical procedures: thyroidectomy, rectal surgery, herniorrhaphy, radical prostatectomy, and partial nephrectomy (Fig. 1). The choice among the 3 different surgical approaches was a joint decision made by the patients and physicians, with all patients being suitable candidates for each surgical approach.

The inclusion criteria for this study included a history of the 55 most common robotic procedures during the period, as well as the corresponding open and laparoscopic (lapa) surgical procedures.
Our hospital conducted its first robotic operation on December 24, 2018. Over the past 3 years, we have made significant advancements, acquiring the da Vinci SP surgical system (Intuitive Surgical, Inc.) as our second robot in 2022 and currently operating 2 robotic systems. Initially, when robotic surgery was introduced at our institution, only the doctor overseeing thyroid procedures had robotic experience. The other surgeons, from various specialties, lacked this experience and participated in a startup program provided by the robot manufacturer, Intuitive. At that time, robotic technology was utilized in 4 departments: surgery, urology, obstetrics and gynecology, and thoracic surgery. Over the past 3 and a half years, the composition and experience level of the staff in these departments have substantially changed. Existing professors have gained proficiency in robotic procedures, and new professors have been recruited and trained to operate these systems.
Outcome Measures
We investigated variables across 3 principal domains. Initially, we assessed the clinical and operational performance changes over a 3.5-year period following the introduction of robotic technology at our hospital. Next, we analyzed the shifts in patient ratios undergoing 3 different surgical procedures in 4 departments responsible for robotic surgery during the same timeframe, to observe changes in patient demographics according to the surgical method postimplementation. Lastly, we conducted a comprehensive evaluation of the operational effectiveness of the robotic implementation, considering local, national, and international contexts. The robotic center team at our hospital evaluated the clinical and operational performance metrics. To facilitate comparisons with other hospitals, the data was deidentified and sent to Intuitive for analysis. Clinical data collection following surgical treatment included both clinical and operational information. Basic demographic and clinical data included patient age, sex, hospitalization day, discharge day, operation day, postoperative length of stay (LOS), and intensive care unit admissions.
Surgical data were extracted from standardized data collection sheets and included surgical modality (robot-assisted, open, and laparoscopy), diagnosis code, procedure code, number of attending physicians, number of attending nurses, operating room minutes, intraoperative complications or conversions to open surgery, bleeding volume during the operation, and the presence of transfusion or surgical site infection.
Statistical Analysis
All patient information was deidentified, and Intuitive received anonymized data from our hospital. The data were processed, and the results were sent back to our hospital after the linked data had been destroyed. The data review board committee of CHA approved this process. The software Prizm 10 (GraphPad, San Diego, CA, USA) was utilized for statistical analysis and graph production. Outcome variables were compared using analysis of variance, followed by the Holm-Sidak multiple comparisons test when appropriate. Results were considered statistically significant if the null hypothesis probability was less than 5% (P<0.05). Data were not collected as part of a formalized clinical study and were not case-matched for patient complexity and/or disease status, which may have affected comparability across different surgical modalities. Therefore, the data should be regarded as informational only and not conclusive. Operating room minutes were recorded from wheels-in to wheels-out. Individual outcomes may have varied based on several factors, including but not limited to, patient characteristics, disease characteristics, and surgeon experience.
RESULTS
We analyzed EMR information from 3,147 patients who underwent surgical treatment using the da Vinci Xi surgical system (Intuitive Surgical, Inc.). These operations, performed using robot-assisted, laparoscopic, and open techniques, spanned 5 different procedures. The data collection period was from January 1, 2019 to June 30, 2022.
Table 1 presents clinical and operational information for all patients. The volume of data was so extensive that it was impractical to discuss all analytical results. To highlight only the statistically significant variables, robotic surgery in rectal resection showed a shorter LOS than open surgery. Additionally, the number of attending nurses and physicians was generally lower for robotic surgery across most procedures, suggesting reduced surgery-related human resource costs (Table 1). The data related to herniorrhaphy in this table were deemed unsuitable for interpretation due to the inclusion of operations performed alongside other procedures.

Clinical and operational performance information for all patients during the study period
The previous results are drawn from an internal hospital analysis; from this point, we will discuss the findings from CHA’s external analysis. This external analysis differed from our internal review in 2 key ways. First, it introduced a fresh perspective on robotic surgery, emphasizing the gradual acquisition of technical expertise by surgeons. Second, the analysis proved extremely valuable by providing insights into the hospital’s current state and potential trajectory, comparing our robotic surgery outcomes with those from external facilities that perform robot-assisted procedures.
Fig. 2 shows the changes in surgical metrics for robotic procedures over 3 and a half years following the implementation of the robotic system. Thyroid surgery, which was performed by a single surgeon, showed a consistent decrease in both surgery duration and blood loss (Fig. 2A and D). Prostate cancer surgery, conducted by a team of 4 surgeons, also demonstrated reductions in these metrics as the surgeons gained experience (Fig. 2B and E). Partial nephrectomy, performed by 3 urologists, showed decreased operation time and blood loss for the two who started the procedure initially, whereas the metrics for the urologist who joined in 2021 showed an upward trend (Fig. 2C and F).
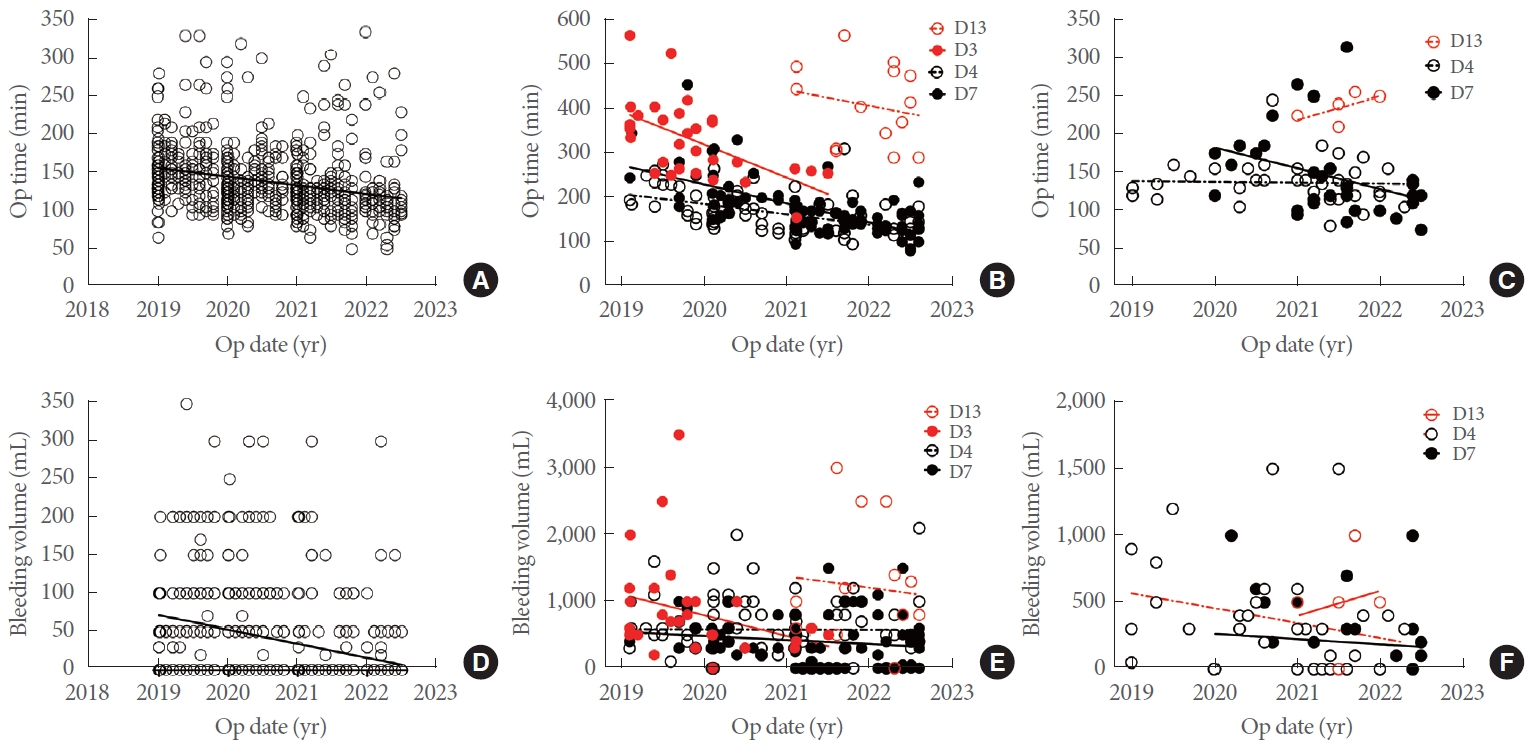
Changes in operation time (A, B, C) and the amount of blood loss (D, E, F) for each type of robotic surgery performed by a single surgeon over time. (A, D) Thyroidectomy. (B, E) Radical prostatectomy. (C, F) Partial nephrectomy. Op, operation.
An analysis of the robotic operations during the first 2.5-year revealed that each department functioned independently without centralized coordination, leading to unoccupied slots on Mondays, Wednesdays, and Fridays. The robotics center later allowed surgeons to adjust their outpatient and surgical schedules while implementing centralized changes to ensure full utilization of specific weekdays (Fig. 3). The surgeons at our institution successfully adapted to robotic surgery in terms of robotic surgical techniques over the course of 3 and a half years, as evidenced by the fact that the console time is currently shorter than the national average However, the effectiveness of robotic surgery continues to require long-term monitoring and communication with surgeons, especially since our institution utilizes more devices for robotic surgery than the national average. Even our most skilled thyroid surgeons used more instruments than average (Fig. 4).

Daily average rate of equipment utilization for the week. (A) Fourth quarter, 2021. In 2021, fewer than 40% of robotic surgeries were scheduled on Mondays, Wednesdays, and Friday. (B) Fourth quarter, 2023. In contrast, all daily schedules were over 70% full due to coordinated changes made by the robotic center.

Comparison of our surgeons with those at other institutions nationwide based on robotic console time and the number of arms used per surgery. Across all procedure types, our surgeons generally required less time than the national average. However, the number of arms utilized in some procedures was higher than the national norm, suggesting the need for ongoing monitoring of these findings. (A) Thyroidectomy. (B) Radical prostatectomy. (C) Partial nephrectomy. (D) Rectal resection. (E) Inguinal herniorrhaphy. This figure is based on Intuitive’s internal data for 2022.
Given the higher costs of robotic surgery compared to traditional surgery, there were worries about the potential increase in the number of robotic procedures when it was initially introduced at our hospital. However, an analysis focusing only on the fields of urology and thyroid surgery during the last 3 and a half years has proven otherwise. After the introduction of robotic surgery, the frequency of surgery performed using conventional methods either remained constant or increased. In addition, the implementation of robotic surgery has led to a significant increase in the total number of patients undergoing treatment for each disease at our hospital. Specifically, there has been a 4.4-fold increase in patients receiving treatment for urologic oncology and a 1.7-fold increase for thyroid cancer (Fig. 5A and B). Our hospital is located in Incheon, Korea, which is home to 3 university hospitals. Hence, it might be reasonable to establish an objective that our hospital would handle one-third, or approximately 30%, of these cases in the local region. The proportion of surgical procedures performed at our hospital for each disease in Incheon, which was previously low, has increased by 12.4% for urologic oncology and 11.4% for thyroid cancer in the 3 and a half years since the introduction of robot surgery (Fig. 5D and E). There was a significant increase in the overall number of total soft tissue operations, increasing from 2,746 to 3,163, within a span of 3 and a half years following the implementation of the robotic system, as compared to the period before its introduction (Fig. 5C). The percentage of these operations carried out at our hospital relative to all operations in the Incheon area rose from 17% to 20% (Fig. 5F). Considering the context of our hospital’s location in Incheon, I believe that the hospital still has the potential to expand by roughly 10% in this regard.

The impact of robot implementation on patient inflow over time. This figure illustrates the changes in patient inflow (A, B, C) and the corresponding percentages (D, E, F) in the Incheon region, specifically for those who visited Inha University Hospital (Inha) following the implementation of the robot. Panels A and D represent all urologic oncology procedures; panels B and E denote thyroidectomy; panels C and F indicate all soft tissue operations at our hospital. “Conventional” refers to open and laparoscopic surgery. “The others” refers to other hospitals in the Incheon region.
The significance of conducting this CHA analysis for hospitals lies in its potential to improve the existing state of robotic technology in healthcare facilities by facilitating domestic and international comparisons. There is a discrepancy in the number of operations per system between hospitals that introduced robots within the past 5 years and hospitals that have had robots for a longer period. However, we could not conduct a statistical analysis of the corresponding data, which belong to Intuitive. Globally, the mean numbers for hospitals within 5 years of implementation and thereafter are 57.0 and 74.3, respectively. In the domestic context, the mean values are 66.2 and 87.1, respectively (Fig. 6). Our hospital’s surgical volume has increased significantly in both global and domestic comparisons (Fig. 6A and B), climbing from 69 per system in 2019 (less than 5 years) to 109 in 2023 (more than 5 years).

Comparison of our performance with global and national data. This figure illustrates the number of procedures performed by each da Vinci robot system across all hospitals that have implemented the technology worldwide (A) and in South Korea (B) as of the fourth quarter of 2023. The left boxplot shows the frequency of surgeries performed per robot at hospitals that have been operational for less than 5 years since their introduction. The right boxplot presents the corresponding data for hospitals that have been operational for more than 5 years. This figure is based on internal data from Intuitive. Inha, Inha University Hospital; Q1, first quarter; Q4, fourth quarter.
In 2022, our hospital ranked 10th among 84 hospitals nationwide in terms of the number of procedures performed per robot machine (Fig. 7A). Additionally, Fig. 7B shows the number of surgeries associated with each procedure at our hospital in 2022, alongside the 70th and 90th percentiles for all 84 hospitals, indicating the targets for our hospital’s future development. In thyroid surgery, the department has the best performance in the country; however, other departments appear to require a substantially more monitoring and support.

Current and future performance of our hospital’s robotic surgery center in Korea. (A) The number of procedures performed per robotic machine in 84 hospitals across the nation in 2022. (B) The radar chart displays the number of operations associated with each procedure at our hospital in 2022, alongside the number of operations in the 70th and 90th percentiles of all 84 hospitals in our country. This figure is derived from the internal data of Intuitive.
DISCUSSION
This study highlights the importance of developing strategies for hospital robotic surgery over the medium to long term, drawing on integrative analyses from the initial 3–5 years following the implementation of robotic systems in hospitals. It is crucial to leverage this evidence to devise a plan for future hospital-wide transformations and to make incremental progress in this area [13-15]. It is essential to thoroughly evaluate this evidence to strategize for upcoming hospital-wide changes and to advance incrementally in this field [9, 16]. The study provides evidence from hospital-based analyses. However, given that the trajectory of the hospital’s development can be determined by comparing its robotic surgery capabilities with those of other hospitals that have robots, analysis by a global corporation is essential for grasping recent trends. By comparing hospital robot-related activities with those of other robot-implementing hospitals worldwide, this study demonstrated that hospital strategy and the support of the CHA program from the global company Intuitive can improve hospital robot-related activities. Subsequently, our hospital acquired an additional robot, SP, in 2023. As of 2024, it is using 2 robots, conducting approximately 70–80 procedures monthly. These achievements in the 5 years since the introduction of robotic surgery are believed to have been significantly influenced by the internal changes implemented through the CHA program in the third year of robot introduction.
An analysis of robotic surgery performed at our hospital over the past 3 and a half years shows that we have achieved favorable outcomes by implementing diverse modifications and appropriate interventions across all aspects of robotic surgery within the institution. Initially, only the attending professor who conducted thyroid surgery had prior experience with robotic surgery from his previous hospital. The other staff were undergoing their first training in robot surgery. This experienced professor initially provided valuable assistance to other departments’ surgeons who were new to using robots, thereby facilitating their introduction to this technology. When many hospitals implement robotic technology, they face significant challenges due to a lack of expertise among professors who are unfamiliar with robots. Based on our hospital’s experience, having at least one experienced surgeon from the start is beneficial as they can assist other less experienced surgeons in performing robotic surgery. Over the 3 and a half years, the skilled surgeon also showed a tendency for operations to become shorter and for less blood to be lost. Although he was an excellent surgeon initially, his techniques increasingly prioritized patient safety, a trend that other surgeons also began to exhibit. However, in the case of partial nephrectomy, the urology staff, newly hired in 2021, tended to lengthen the operation and cause more blood loss, indicating that more practice and time were needed. Complications associated with robotic surgery depend on the complexity of each procedure [17, 18]. By specifically examining complications related to robotic surgical techniques, it has been determined that the occurrence rate is very low, suggesting that the robotic center plays a significant role in minimizing these complications. In essence, our experience suggests that achieving this goal depends on implementing a monitoring system within the robotic center that ensures the technical proficiency of every surgeon engaged in robotic surgery and facilitates the correction of any issues that may arise. Furthermore, the purpose of the robotic center is to effectively address diverse internal and external environmental changes over time concerning robotic surgery, with the aim of consolidating them under the overarching objective of ensuring patient safety [19-21]. Due to the involvement of multiple surgeons from various departments, scheduling surgeries and outpatient hours is a complex and rigid process [22, 23]. The hospital management serves as the primary go-between for these departments, with the robotics center handling the majority of the coordination [24, 25]. Initially, studies on robotic surgery usage showed that Monday mornings and Friday afternoons were often unoccupied. The influence of the robotic center is evident in the improved surgical rates on specific days of the week.
With the growing adoption of da Vinci systems, hospitals now face the challenge of validating and strategizing the quality of their robotics programs [26-28]. The need for this arises from the necessity to enhance one’s robotic system by benchmarking against hospitals that possess such technology. Our hospital has seen significant improvements in its long-term robotics programs following an initial performance review by the CHA program. For example, the “console time” associated with our hospital’s robot technology was lower than the national and global averages, indicating better performance. However, analysis has shown that increasing patient numbers is essential for our hospital to become the top facility in Korea. To achieve these goals, it is crucial to determine the specific strategic plan needed for recruiting department members. Given that our hospital’s specialist in thyroid surgery has already exceeded the regional objective by 30% in our region, it would be prudent to endorse the formation of a team by augmenting the staff count to complement the professor’s proficiency, rather than raising the workload of surgeries. The Department of Urology, having recently hired young surgeons specializing in robotic surgery, has not yet met its local 30% target. However, as these surgeons gain experience, significant improvements are expected. Consequently, it has been decided that no additional staff are needed to operate the robots. In our view, staffing decisions should be made at the hospital administration level.
The study’s limitations include the superficial and heterogeneous nature of the data, resulting from analyzing multiple departments simultaneously. There is too much data to present in a single publication, so the findings focus on representative diseases and departments. Due to this lack of specificity, the results should be viewed as informative rather than scholarly. Another major concern is the potential legal issues in various countries due to the hospital’s data being analyzed externally by the global corporation Intuitive [29, 30]. This issue was addressed by deidentifying the data and disposing of it post-analysis, as advised by our hospital’s legal team. Despite these challenges, the publication of this paper is deemed necessary for standardizing robotic surgery from a management perspective, and it is hoped that promoting fair competition among global hospitals will improve patient safety. Privacy regulations in Korea are particularly strict [30], posing additional challenges for this type of research. Given the different legal frameworks regarding personal data across countries, future studies will likely need to address these issues specifically. Interestingly, while similar analyses have been conducted in the United States, none have been published. Our institution is the first in Asia to undertake and publish such a study.
As more hospitals are implementing robots, increasingly many hospitals are in the early phases of robot adoption and preparing for the subsequent phase. Among the challenges that hospitals face when implementing robots, the most significant is the pressure to succeed following substantial investments. As the number of hospitals encountering these challenges increases, conducting research on this topic becomes crucial to guide the development of hospital strategies by comparing them with experienced institutions. This will enable fair competition in the global market for robotic surgery, ultimately improving patient safety. The aim of this study is not to promote our hospital’s achievements but to offer insights based on our experiences to assist other hospitals in addressing the initial challenges of robot deployment. Another critical aspect of this study is the need for a comprehensive international evaluation of hospital performances, which requires prompt attention to legal issues in each country.
Notes
Grant/Fund Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Research Ethics
It was confirmed that this process complied with Korea’s Personal Information Act, as verified by Institutional Review Board (IRB) of the Inha University Hospital. The Inha Ethics Committee granted ethics approval (IRB protocol number: 2022-12-017-000).
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
· Conceptualization: JWY, TL
· Data curation: MSJ, YMK
· Formal analysis: SPC, MSJ, JWY
· Methodology: SKC, JWY
· Project administration: JWY, TL
· Visualization: SPC, MSJ
· Writing - original draft: SPC, JWY
· Writing - review & editing: JWY, TL