INTRODUCTION
Spina bifida is a type of neural tube defect that occurs due to abnormal fusion of the caudal neural tube during early development. This defect affects the central nervous system and can lead to permanent disability. As the most common birth defect, its incidence rate ranges from 1 to 10 per 1,000 live births [1]. Magnetic resonance imaging can facilitate early diagnosis, and untethering procedures may help reduce potential lifelong disabilities. Spina bifida can cause severe disability across multiple organ systems, including neurological deficits, sphincter dysfunction, and limb deformities [2].
The ability of a patient to store and empty urine can be impacted by variations in the somatic, parasympathetic, and sympathetic innervation of the bladder, potentially leading to chronic kidney disease due to impaired bladder dynamics. Given the close connection between the lower urinary tract (LUT) and the autonomic nervous system (ANS) [3], an indicator of ANS activity could provide objective data about bladder sensations and enhance our understanding of the underlying pathophysiology of specific diseases. Previous studies have examined baseline values and changes in ANS activity during bladder filling in healthy controls or patients with LUT symptoms (LUTS) without neurological deficits [4,5]. However, no studies have yet explored how the ANS influences bladder pathophysiology in patients with spina bifida.
Assessing heart rate variability (HRV) is one of the most practical, reproducible, and noninvasive methods for monitoring the ANS. HRV is used to quantify the spontaneous fluctuations in the R-R interval of a continuous electrocardiogram (ECG) in response to physiologic demand, reflecting the ongoing interplay between sympathetic and parasympathetic influences [6]. While HRV was initially employed to assess autonomic function in cardiovascular diseases, it has also been utilized in several studies to evaluate underlying ANS dysfunction related to LUT disease [5,7,8]. Consequently, our study objectives were twofold: (1) to compare ANS activity, as measured by HRV, between children with spina bifida and a control group at baseline, and (2) to examine and compare responses to bladder filling during urodynamic studies between groups.
MATERIALS AND METHODS
A retrospective pilot study was conducted between July 2015 and March 2016. This study was used to validate the method of HRV measurement and to identify differences between the control group and the patients with spina bifida. Subsequently, a prospective study was carried out from April 2016 to February 2017 to supplement the retrospective data, after the study protocol received institutional review board approval. Participants were informed about the study’s purpose and procedures before participating, and they were made aware that they could withdraw from the study at any time without explanation. In both the pilot and prospective studies, informed consent was obtained from the parents as well as the children, the latter through an age-appropriate agreement document in the presence of their parents or legal representatives. The inclusion and exclusion criteria of the prospective protocol were retrospectively applied to the pilot data. Regardless of when the study was conducted, HRV was measured using a consistent protocol during the video-urodynamic study.
Patient Selection
All patients underwent an evaluation that included a clinical history, a physical examination, and a questionnaire regarding LUTS. The study group was comprised of patients older than 4 years who had undergone detethering surgery due to spina bifida, due to either a lipomeningomyelocele or a meningomyelocele. The control group consisted of patients who had undergone video-urodynamic study to assess vesicoureteral reflux (VUR) or other upper urinary tract anomalies. The exclusion criteria were as follows: use of anticholinergics and alpha-blockers within the prior month; diagnosis of neurological disorders affecting the ANS, excluding spina bifida; diagnosis of hypertension or arrhythmia; diabetes; history of previous urological surgery, including augmentation cystoplasty; anatomical abnormalities in the bladder and urethra; and consumption of coffee, tea, cigarettes, or other foods that could affect the ANS prior to examination. In the control group, patients who exhibited LUTS such as daytime incontinence or urgency were also excluded.
In the pilot study, 16 cases were initially considered. However, 4 patients were retrospectively excluded based on criteria related to LUTS that necessitated medication. Additionally, 5 cases involving spina bifida were excluded due to a history of augmentation cystoplasty and the use of anticholinergics. The remaining 7 patients were retrospectively recruited. Starting from April 2016, 20 patients were prospectively screened for inclusion in the study, and 13 were ultimately enrolled. The final analysis included a total of 20 children, with 9 in the control group and 11 in the study group.
Urodynamic Studies and HRV Measurements
Urodynamic study was conducted using a technique recommended by the International Children’s Continence Society [9]. We employed 6F double-lumen catheters for the urethra and 12F fluid-filled balloon catheters for the rectum. A saline solution, warmed to body temperature, was infused at filling rates of 5%–10% of a known or predicted capacity. The anticipated bladder capacity was calculated using the following formula (in mL): [30+(age in years × 30)]. For children with spina bifida, bladder filling was halted under the following conditions: if the child expressed a strong urge to void, if continuous leakage was observed, if detrusor pressure exceeded 40 cm H2O, or if the patient reported a sensation of bladder fullness or abdominal discomfort [10]. The patients were examined in the supine position without anesthesia. Surface electrodes were utilized, and EMG patches were symmetrically positioned perineally, to the left and right of the anus.
In the control group, bladder filling was sustained until the children experienced a strong desire to void and could no longer postpone micturition. The maximal cystometric capacity referred to the bladder volume at the conclusion of the filling phase or when “permission to void” was granted [9].
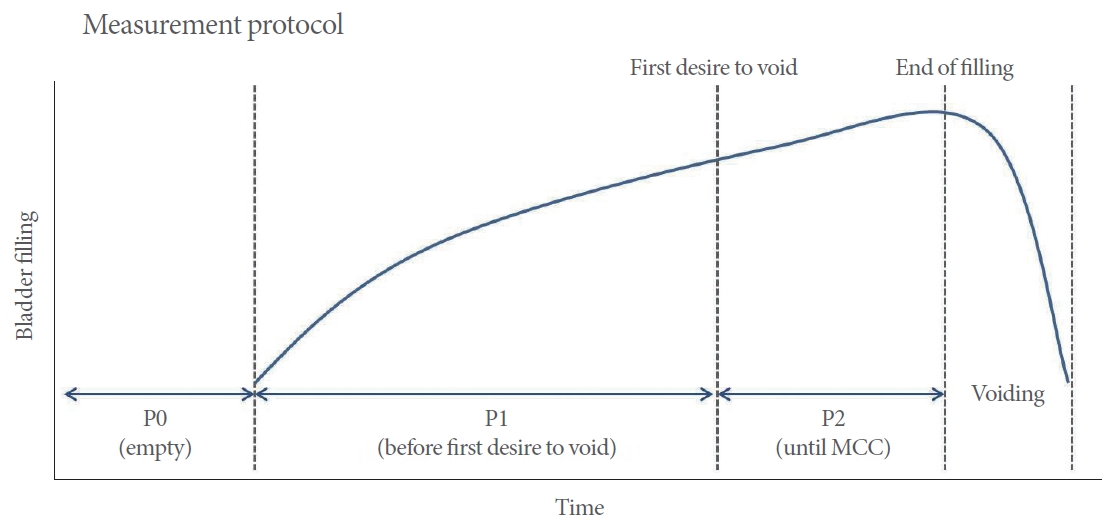
To ensure that anxiety induced by the examination did not influence baseline HRV levels, patients were provided with ample stability following the setup of the examination. After the setup and calibration of the 3 urodynamic channels, continuous HRV data were collected during 3 distinct periods of bladder filling (Fig. 1).
The present study compared R-R intervals obtained from a tablet computer with those derived from the Polar H7 chest belt heart rate monitor, which served as the reference (Polar Electro Oy, Kempele, Finland) and had been previously validated [11]. The R-R values were transmitted to the computer through the Elite HRV application (Elite HRV LLC, Asheville, NC, USA) and then exported for HRV analysis using the Kubios HRV standard version 3 software (Kubios Oy, Kuopio, Finland). Both time and frequency domain measures were evaluated in accordance with existing guidelines [12]. In line with most studies, the time domain measures included (1) the standard deviation of all NN intervals (SDNN), (2) the root mean square of successive differences of successive R-R normal intervals (RMSSD), and (3) the percentage of successive R-R interval differences exceeding 50 msec (pNN50). Both RMSSD and pNN50 are associated with high frequency (HF), which reflects changes in parasympathetic activity. The frequency domain involved power spectra calculations with the integration of (1) very low frequency [LF] ( ≤ 0.04 Hz); (2) LF (0.04–0.15 Hz), which primarily indicates sympathetic cardiac modulation with some parasympathetic influence; (3) HF (0.15–0.4 Hz), which signifies parasympathetic modulation; and (4) the LF/HF ratio, which serves as a measure of the autonomic balance between the sympathetic and parasympathetic nervous systems [12].
Statistical Analysis
Data are presented as the mean ± standard deviation. The Mann-Whitney U-test was employed to compare mean values using a nonparametric approach, while the t-test was utilized for parametric variables. The coefficient of variation (CoV) was calculated (using the formula CoV = standard deviation/mean) to assess the dispersion of a probability distribution. Changes in HRV during bladder filling were compared within each group using repeated-measures analysis of variance. The assumption of compound symmetry was evaluated using the Mauchly sphericity test. Upon identifying the significance of the Mauchly sphericity test and noting the absence of spherical or posite symmetry in repeated measurements of HRV parameters, the Pillai trace multivariate test was implemented. The mean value of each HRV parameter across different time periods was compared using a paired t-test. All calculations were performed using IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA), with the significance threshold set at P ≤ 0.05.
RESULTS
No significant differences were noted between the 2 groups in terms of baseline characteristics (Table 1). The control group consisted of 7 patients who had previously been diagnosed with VUR and 2 patients who were undergoing evaluation to determine the presence of VUR. In the study group, 7 patients (63.6%) were utilizing clean intermittent catheterization. Low bladder compliance, defined as less than 20 mL/cmH 2O, was observed in 7 patients (63.6%) from the study group, while no such cases were found in the control group.
Baseline time domain parameters indicated that the patients with spina bifida exhibited a significantly reduced mean RMSSD (25.64 msec vs. 48.22 msec, P = 0.015) in comparison to the control group (Table 2). These patients also demonstrated a decreased pNN50 (7.33% vs. 29.48%, P = 0.021). Within the frequency domain, the HF was lower in patients with spina bifida (125 vs. 776, P = 0.003), although no significant difference was observed in the LF. The LF/HF ratio at baseline was significantly higher in the children with spina bifida compared to the control participants (5.04 vs. 0.67, P = 0.014).
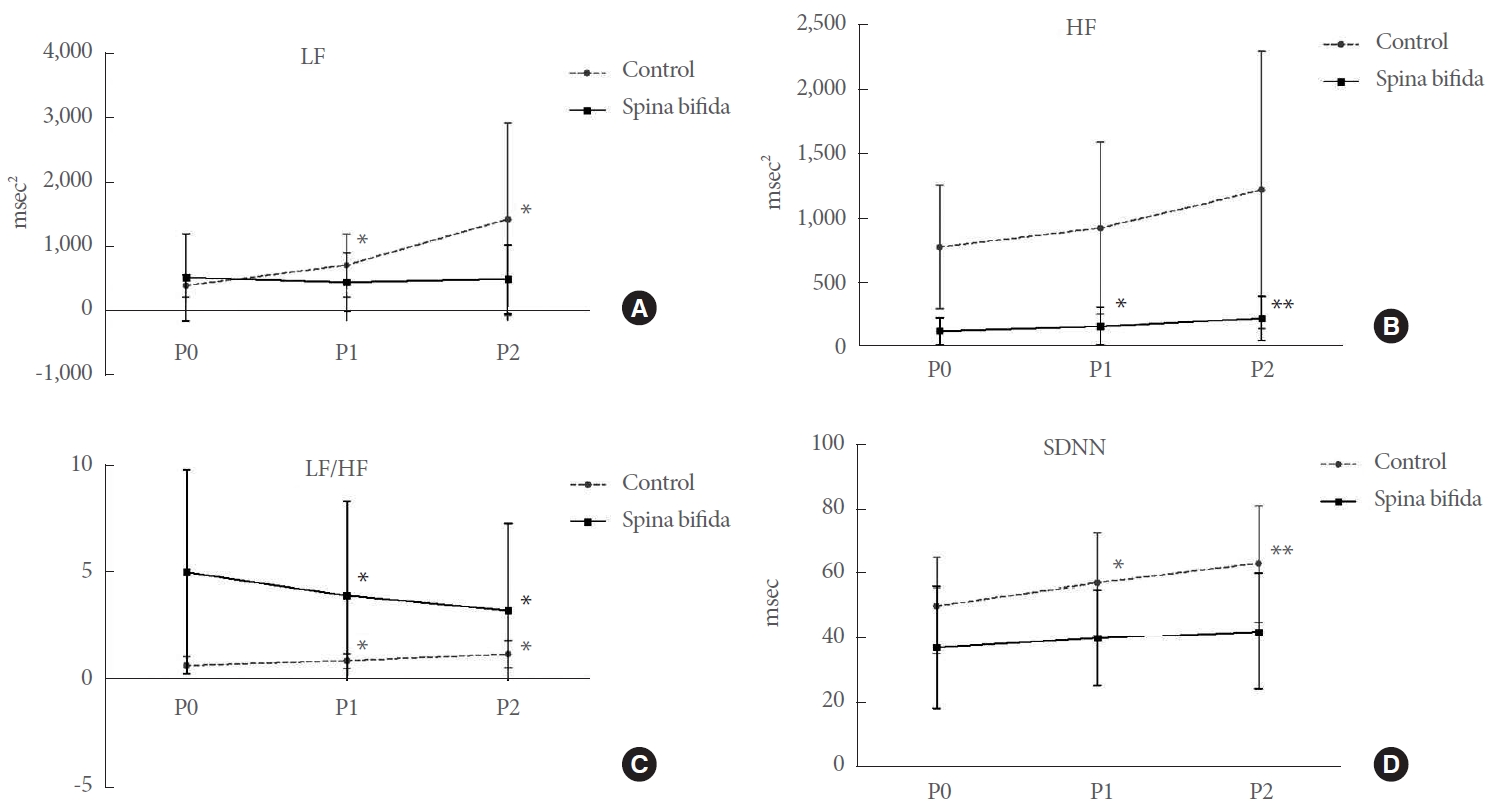
Table 3 illustrates the relative changes in HRV parameters from the baseline to the bladder filling period. The heart rate remained consistent during bladder filling in both groups. However, several HRV parameters exhibited a tendency to increase or decrease during bladder filling. In the time domain, a statistically significant difference was observed in SDNN values, but only in the control group (Fig. 2). LF values displayed an upward trend with bladder filling in the control group. HF increased only in patients with spina bifida, although the difference was not substantial (P0 = 125.08 ± 104.39 vs. P2 = 223.10 ± 169.90; P = 0.002). The LF/HF ratio changes showed an increase in the control group (P0 = 0.67 ± 0.42 vs. P2 = 1.21 ± 0.64; P = 0.018) and a decrease in the spina bifida study group (P0 = 5.04 ± 4.75 vs. P2 = 3.26 ± 4.03; P < 0.001).
DISCUSSION
To our knowledge, this study is the first to objectively compare the baseline profile of ANS activity and responses to bladder filling in children with and without spina bifida, utilizing the spectral analysis of cardiovascular signal variability methodology. This study produced several noteworthy findings. First, the baseline profile of HRV was altered in patients with spina bifida, characterized by decreased values associated with the peripheral nervous system (RMSSD, pNN50, and HF) and an increased LF/HF ratio, indicative of sympathetic dominance. The response to bladder filling also significantly differed between the groups, most notably in the LF/HF ratio (with an increasing value in the control group versus a decreasing value in the spina bifida group with bladder filling). These findings offer insight into the underlying neuropathology of spina bifida.
The severity and location of the fusion abnormality can lead to a range of urological consequences. Most commonly, an upper motor neuron lesion with detrusor overactivity and detrusor sphincter dyssynergy may develop. However, an acontractile detrusor and sphincter denervation can also occur as a result of spinal cord tethering [13,14]. The primary treatment for spina bifida remains a combination of pharmacological agents and clean intermittent catheterization, though this approach has achieved only limited success [15]. Current treatment strategies are focused more on preventing the consequences of neurogenic bladder, rather than enhancing our understanding of the disease. Consequently, our comprehension of the disease has not substantially improved.
Since Hon and Lee [16] initial report on HRV changes, HRV has been widely utilized as a quantitative indicator of ANS activity. Prior research has shown that ANS dysfunction, as evidenced by HRV, mirrors the underlying pathology of LUTS [5,8]. The most studied LUT associated with HRV is overactive bladder (OAB). However, the results and study settings examining how ANS differs from healthy controls have been inconsistent, making this a debated area of study. Hubeaux et al. [17] reported a predominance of parasympathetic activity when the bladder was empty and a surge of sympathetic activity at the end of bladder filling in women with OAB syndrome. Choi et al. [18] noted a decrease in HRV indices, including HF, SDNN, and RMSSD, in women diagnosed with OAB compared to healthy women. In children with bladder bowel dysfunction, HF was significantly lower than in healthy controls at baseline [19].
In healthy individuals, the LF/HF ratio maintained a stable sympathovagal balance until the initial desire to void. However, this balance shifted towards sympathetic activation prior to a strong urge to void [4]. This response is thought to be triggered by a mechanism akin to the vesicovascular response, which is mediated by sympathetic nerves such as the hypogastric nerve [20]. Contrary to previous studies, our research found that the LF/HF ratio increased until the first desire to void and continued to escalate until the completion of bladder filling. This outcome could be attributed to the younger age group in our study, who may not have been able to fully express their bladder sensations, as well as the broad variation in HRV value. During bladder filling, the spina bifida group, unlike the control group, exhibited an increase in HF without a corresponding increase in LF, leading to a decrease in the LF/HF ratio. These findings indicate ANS dysfunction, predominantly sympathetic, in individuals with spina bifida. Considering that the thoracolumbar sympathetic efferent pathways in the hypogastric and pelvic nerves suppress detrusor muscle activity and stimulate the bladder base and urethra, the observed changes in sympathetic activity during bladder filling could result in an urgency sensation and issues with urine storage. In our study, neurogenic detrusor overactivity was identified in only 4 patients (36.3%); however, previous urodynamic studies have reported this condition in all but 1 patient. These urodynamic findings may be linked to the reduced LF/HF ratio during bladder filling.
In the time domain, SDNN significantly increased with bladder filling in the control group, while it remained unchanged in patients with spina bifida. Considering that SDNN represents overall HRV [12], the unchanged SDNN value in spina bifida patients could be attributed to a decrease in ANS neurotransmission during bladder filling. Drawing parallels from the enteric nervous system, which shares a similar nerve distribution with the bladder, we observed neural loss and a decrease in nerve fiber density in the myenteric plexus in patients with spina bifida. This correlated with the severity of bowel dysfunction [21]. These changes may be a response to disrupted extrinsic innervation, leading to trans-neuronal degeneration. Consequently, we hypothesize that these findings may be associated with an overall decrease in HRV value during bladder filling in spina bifida. However, they do not provide an explanation for the sympathetic predominance observed at baseline.
Recently, an evaluation of autonomic cardiovascular function was conducted in children with meningomyelocele who use wheelchairs. The results showed a reduction in RMSSD at rest compared to the control group, which aligns with our findings of decreased RMSSD, pNN50, and HF in the spina bifida group at baseline [22]. The pathology leading to a diminished vagal tone and an increased LF/HF ratio in patients with spina bifida remains unclear. In patients who have experienced thoracic spinal cord injuries, cases have been documented of elevated heart rates and decreased vagal tone [23]. This may reflect compensation for decreased stroke volume and compensatory reductions in vagal tone to maintain autonomic balance [24,25]. Patients with spina bifida have been found to exhibit deteriorating vascular properties, including small diameter, low flow, and high shear stress [26]. These findings suggest that the decrease in vagal tone and the predominance of sympathetic activity in spina bifida may occur through a mechanism similar to that observed in spinal cord injury.
The primary limitation of this study was the small sample size, which precluded the performance of HRV analysis for each subtype according to the urodynamic study. Given the substantial deviation of baseline HRV, a larger study is necessary to validate our findings. Another limitation was that HRV measurements in our study were conducted using a nonmedical Bluetooth device, rather than conventional ECG. However, recent studies have indicated that Bluetooth devices can provide a satisfactory level of agreement for HRV measurement relative to ECG, thus validating the measurement method used in this study [11,27]. While other criteria could be considered to reflect changes in HRV over time, it is challenging to divide periods based on a specific time due to the varying bladder filling times inherent to each patient’s bladder capacity. Patients with spina bifida often lose their sense of bladder fullness and exhibit bladder underactivity, which can complicate the determination of the appropriate point for each period. Despite these limitations, the criteria we used to divide each period may be an (admittedly suboptimal) method for observing the trends of HRV changes during bladder filling in both control and spina bifida groups. Another potential concern is that HRV may be influenced by emotional stress induced by the artificial setting of the study. However, the same setting was applied to both groups, and the examination was conducted with ample time for adaptation. An additional limitation could be that the control group was composed of children with VUR, who may have abnormal bladder dysfunction that could be related to HRV, although this has not been studied.
At baseline, HRV parameters representing peripheral nervous system activity were found to be reduced in children with spina bifida in comparison to the control group. During bladder filling, a relative increase was noted in parasympathetic activity, with constant sympathetic activity observed in children with spina bifida. In contrast, the control group exhibited a shift in the balance of sympathetic and parasympathetic activities, favoring the sympathetic component. These findings could be associated with the underlying neuropathology induced by spina bifida, and this information could potentially be utilized to enhance our understanding and management of this condition.