INTRODUCTION
Overactive bladder (OAB) syndrome is defined by the International Continence Society as urgency, with or without incontinence, usually associated with urinary frequency and nocturia. Some papers have reported that the prevalence rate for men with OAB is higher in some Asian countries than in Europe, the USA, and Canada [1-3]. OAB was reported to be significantly associated with an increased prevalence of erectile dysfunction, and reduced sexual activity and satisfaction due to lower urinary tract symptoms (LUTS) [4,5].
Mirabegron, a selective beta-3 adrenoceptor agonist, is the first drug of its type to be clinically available for the treatment of OAB. Beta-3 adrenoceptors are the predominant beta receptors expressed on detrusor smooth muscle cells, and their stimulation is thought to induce detrusor relaxation. In addition, the activation of beta-3 adrenoceptors initiates relaxation of strips from the corpus cavernosum (CC) in humans and rats via the nitric oxide (NO)-cyclic guanosine monophosphate (cGMP) signaling pathway [6]. A previous study proposed that erectile function (EF) was improved by neurogenic relaxation after intracavernous administration of mirabegron in diabetic rats [7]. In previous human studies, 2 research groups demonstrated that mirabegron improves both OAB symptoms and EF in male OAB patients without serious adverse effects [8,9]. In 1 systemic review article, combination therapy of phosphodiesterase type 5 inhibitor (PDE5I) and mirabegron showed significant improvement on urological symptom scores or quality of life (QoL) compared to PDE5I therapy only [10]. Nevertheless, nearly all of the reviews did not explicitly state the effect of mirabegron on sexual function.
According to the updated treatment guidelines published by the American Urological Association and European Association of Urology, behavioral therapy is considered the first-line treatment for patients with OAB, followed by pharmacotherapy. However, one earlier study has shown that combining behavioral and drug therapy yields greater improvements in OAB symptoms compared with drug therapy alone [11]. However, there was no report on male EF and ejaculatory function in OAB patients in that randomized controlled trial (RCT). Consequently, in the present study, we aimed to evaluate the effectiveness of behavioral therapy alone and a combination of behavioral therapy and mirabegron medication for reducing OAB symptoms and effects on sexual function in male OAB patients.
MATERIALS AND METHODS
Recruitment and Allocation
Sexually active men aged Ōēź 20 years old with OAB symptoms were enrolled between June 2020 and May 2022. The overactive bladder symptoms score (OABSS) questionnaire was used to diagnose OAB; a positive diagnosis was considered if the OABSS urgency score was Ōēź 2 and the sum scores were Ōēź 3. These recruited patients should be able to have sexual activity during study period. Written informed consent was obtained from the participants prior to their inclusion within the study. This trial followed the CONSORT (Consolidated Standards of Reporting Trials) guidelines (Fig. 1).
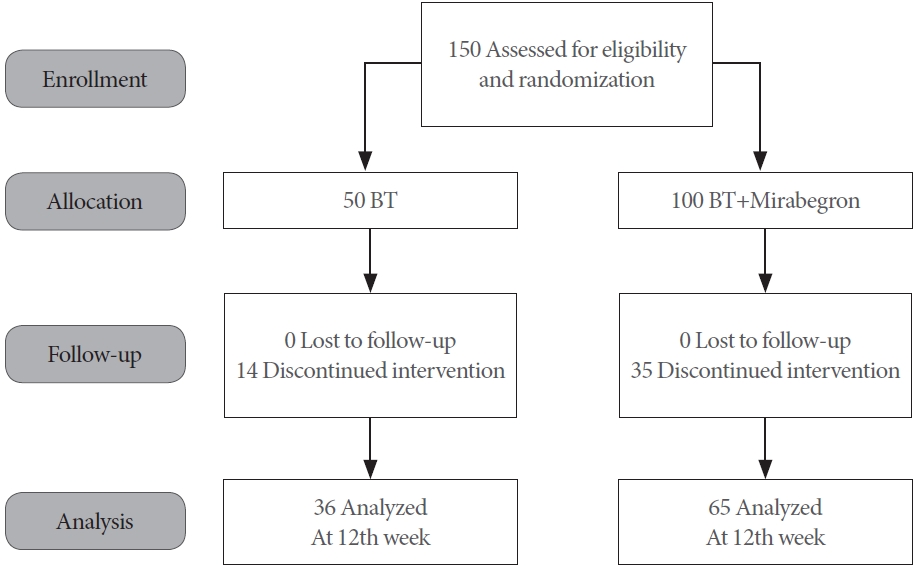
A total of 150 patients were recruited and allocated into the 2 study subgroups in a 2:1 ratio. The 2 study subgroups were ŌĆ£combined behavioral therapy and mirabegronŌĆØ and ŌĆ£behavioral therapy aloneŌĆØ (Fig. 2). The permuted block randomization method was used and each randomization number was assigned according to the time-sequence for when the screened patient became eligible for inclusion.
The exclusion criteria were concurrent use of phosphodiesterase type 5 inhibitor (PDE5I) or testosterone therapy during the study period, a history of stress urinary incontinence, evidence of an active urinary tract infection or urinary tract stone, confirmed genitourinary tract or pelvic malignancy, genitourinary tract operation during 3 months prior to baseline, postvoid residual urine (PVR) volume Ōēź 100 mL, history of uncontrolled hypertension (systolic > 180 mmHg and/or diastolic > 110 mmHg), history of intolerance to mirabegron, and a history of intravesical onabotulinum toxin A treatment within the last 6 months.
Study Protocol
After randomization, all patients in both groups received 12 weeks of behavioral therapy, urge control strategy, conducted by verbal instruction of each physician investigators or nurse practitioners at baseline visit. The urge control strategy consisted of a reduction in fluid intake at specific times, avoidance of caffeine and alcohol, usage of relaxed and double-voiding techniques, urethral milking, distraction techniques, and bladder retraining to increase bladder capacity and the time interval between voids. In addition, avoidance or substitution of medications with urinary effects, and treatment for constipation were recommended. In second visit, success or failure with bladder control strategies discussed in detail to improve results and adherence.
In the combination subgroup, all participants received mirabegron 50 mg once daily for 12 weeks in addition to the behavioral therapy. In both subgroups, patients who were previously prescribed alpha-blockers and/or 5-alpha reductase inhibitors continued to receive their medication.
Evaluating Parameters and Outcomes
All participants received a thorough urological check-up before they started treatment. This included taking a history of all personal underlying diseases, measuring serum prostate-specific antigen (PSA) levels, a transrectal sonography of the prostate to measure prostate size, completion of the International Prostate Symptom Score (IPSS) questionnaire, a uroflowmetry test, completion of a 3-day voiding diary and measurement of PVR volume by ultrasonography.
There were 2 primary outcomes in this study; the first was change in OAB symptoms as determined by the OABSS, and the second was change in sexual function as determined by the abridged 5-item version of the International Index of Erectile Function (IIEF-5). The others were secondary outcomes, such as patient perception of bladder condition (PPBC) and QoL, and the Male Sexual Health Questionnaire - Ejaculatory Domain (MSHQ-EjD) Short Form. The therapeutic outcomes (IPSS, OABSS, PPBC, QoL, IIEF-5, maximum flow rate, and PVR volume) were assessed at baseline, 4 weeks, and 12 weeks. All outcome measures were assessed and scored in a blinded fashion and all adverse effects were recorded.
Power Analysis
Based on our previous publication [12], the IIEF-5 score decreased from 16.4 ┬▒ 5.5 to 15.6 ┬▒ 5.6 (P = 0.106) and 14.9 ┬▒ 5.9 (P = 0.077) at 4- and 12-week follow-up, respectively. Group sample sizes of 78 and 37 achieve 80% power to detect a difference of 2.600 in a design with 3 repeated measurements having a compound symmetry covariance structure when the standard deviation (SD) is 5.600, the correlation between observations on the same subject is 0.500, and the alpha level is 0.050. With 30% drop out rate, the estimated sample size would be around 150.
Statistical Analysis
All data are described as the mean ┬▒ SD for continuous variables or as n with percentage for categorical variables. P < 0.05 was considered to indicate a statistically significant difference. All changes in symptom scores, including IPSS, IIEF-5, OABSS, QoL, uroflowmetry parameters, and PVR volume were recorded at baseline and at every subsequent visit. All statistical analyses were performed using SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
A total of 100 patients were allocated into the combined behavioral therapy and mirabegron subgroup however 35 (35%) withdrew during the 12 weeks of treatment. A total of 50 patients were allocated into the behavioral therapy alone subgroup however 14 (28%) withdrew during the 12 weeks of treatment (Fig. 1). There was no statistically significant difference in the age, prostate size, PSA level, and testosterone level at baseline between the 2 groups (Table 1). Furthermore, the percentage of comorbidity and prescription of alpha-blockers and 5╬▒ reductase inhibitors were not significantly different between the 2 groups.
There was no statistically significant difference in OABSS, urodynamic parameters, PPBC, 3-day voiding diary, and IPSS at baseline between the 2 subgroups (Table 2). The OABSS questionnaire showed a significant improvement for all symptoms and the total score 4 weeks after combination treatment (Table 2). In the behavioral therapy alone group, total score for the OABSS also showed a statistically significant improvement (from 8.1 ┬▒ 2.7 to 6.5 ┬▒ 2.0, P = 0.011) after 4 weeks treatment; OABSS nocturia (from 2.2 ┬▒ 0.9 to 1.7 ┬▒ 1.2, P = 0.022) and urgency subscores (from 3.5 ┬▒ 1.4 to 2.8 ┬▒ 2.0, P = 0.035) also showed a significant improvement after 12 weeks of treatment. However, the OABSS frequency subscore showed no significant improvement after behavioral therapy alone. Bladder capacity in the combination subgroup was significantly increased after mirabegron (4 weeks and 12 weeks) treatment. However, in the behavioral therapy only subgroup, there was no significant difference in bladder capacity after 12 weeks of therapy.
The functional bladder capacity as determined by the voiding diary, revealed no significant increase after both treatment approaches (Table 2). In the behavioral therapy alone subgroup, all parameters in the 3-day voiding diary, except for daytime frequency, showed no significant change after treatment. Whereas the combination subgroup reported a statistically significant decrease in voiding times (daytime from 8.8 ┬▒ 3.4 to 7.9 ┬▒ 2.3, P = 0.044; night time from 1.5 ┬▒ 1.0 to 1.2 ┬▒ 0.8, P = 0.041) after 12 weeks treatment. Both the behavior only and combination subgroups revealed a significant improvement in bladder condition as measured by the PPBC (from 2.4 ┬▒ 1.2 to 1.5 ┬▒ 1.1, P = 0.001; from 2.6 ┬▒ 1.2 to 1.4 ┬▒ 1.0, P < 0.001, respectively).
IPSS total score, QoL, and voiding subscores showed statistically significant decreases after 4 weeks of treatment in both the behavior only and combination subgroups (Table 2). The combination subgroup had a significantly lower nocturia subscore at 4 weeks compared with the behavior only subgroup. Interestingly, there was no significant difference in the treatment effect after 12 weeks of treatment between the combination subgroup and the behavior only subgroup (storage subscore, 4.4 ┬▒ 2.5 and 4.9 ┬▒ 2.8, P = 0.376, nocturia subscore, 1.5 ┬▒ 1.0 and 1.7 ┬▒ 1.1, P = 0.373).
As for erectile and ejaculatory functions, there were no significant changes in the IIEF-5 score, and the 4 items of the MSHQ-EjD short form in both subgroups at 4 weeks and 12 weeks compared with baseline (Table 3).
DISCUSSION
Behavioral therapy along with pelvic floor muscle training and urge suppression strategies, are recognized by treatment guidelines as a conservative first-line therapy for OAB [13-15]. As shown by previous studies, the advantages of behavioral therapy are avoidance of adverse effects and the effective reduction of OAB symptoms, especially urgency urinary incontinence and urinary frequency, by counseling patients to control urgency and inhibit detrusor contractions [16,17]. In most studies regarding behavioral therapy, researchers demonstrated that a combination of behavior and drug therapy had an additive effect for improving OAB symptoms such as urgency and urinary frequency [11,17-19]. While there are more strong evidences for the use of combination therapy in women, the effectiveness of combined behavioral and drug therapy for men is less clear [18,20-22]. Recently, some studies demonstrated that a combination of antimuscarinic medication and behavioral therapy was better than antimuscarinic medication alone for men [11,18,19].
Mirabegron, is an alternative treatment option to antimuscarinics for LUTS associated with OAB [23]. In 1 meta-analysis, Sebastianelli et al. [24] reported that mirabegron 50 mg provides a reduction in urinary frequency, urgency, and urgency urinary incontinence, and an improvement in voided volume and nocturia. Kuo et al. [25] conducted a double blind, 3 arm (placebo, mirabegron, and tolterodine), RCT among Asian countries, and demonstrated that mirabegron 50 mg once daily for 12 weeks was superior to a placebo for increasing voided volume and reducing the frequency of micturition in patients with OAB symptoms. To the best of our knowledge, this study is the first RCT to explore the effect of combined behavioral therapy and mirabegron on male sexual function in addition to an evaluation of OAB symptoms. In this study, a combination of behavioral and drug therapy demonstrated improved effectiveness on the OABSS, PPBC, IPSS, and the voiding diary after 4 weeks treatment compared with behavioral therapy alone. Interestingly, both treatment approaches showed no statistically significant differences in treatment outcomes for OABSS total score, PPBC, and IPSS after 12 weeks treatment.
Furthermore, OAB is considered to have a significant association with reduced sexual activity and enjoyment due to storage symptoms [4]. Irwin et al. demonstrated that patients with OAB (n = 502) have a statistically higher incidence of ED than controls (n = 502) (25.2% vs. 15.6%, P Ōēż 0.05, respectively). Chuang et al. [1] proposed that increased symptom severity was significantly associated with lower sexual QoL in both men and women. Another study demonstrated that the initiation, maintenance and rigidity of a penile erection were under parasympathetic and somatotopic control [7]. Some authors further concluded that the sympathetic nervous system plays an important role in the subsidence and suppression of an erection [26,27]. Cirino et al. [27] demonstrated that ╬▓3-adrenoceptors are localized mostly in the smooth muscle cells of human CC and can mediate a penile erection. In human CC, they reported that activation by a selective ╬▓3-adrenergic receptor agonist (BRL37344), elicited a cGMP-dependent, NO-independent vasorelaxation that was selectively blocked by a specific ╬▓3-receptor antagonist (SR59230A) [27].
On the basis of these findings, Wu et al. [12] conducted a clinical trial to evaluate the EF of sexually active men with OAB after 12-week treatment with mirabegron. They demonstrated that mirabegron treatment significantly improved male OAB symptoms but not male sexual function, like IIEF-5. Unexpectedly, the results revealed that 12 weeks of mirabegron treatment had a significantly negative impact on men with better baseline EF (IIEF-5 Ōēź 17; 11.7% decrease; P = 0.044). There was no improvement in EF after treatment with mirabegron, especially for the patient group with mild ED (mean IIEF-5 scores 16.3 and 17.3, respectively) in our trial which was also based in an Asian country. However, Karakus et al. [8] revealed that mirabegron may improve EF in some patients with OAB in addition to OAB-related symptoms. Elbaz et al. [9] conducted another study which compared the use of mirabegron and tolterodine for the treatment of patients with ED concomitant with LUTS. In their study, mirabegron resulted in increased improvements in urinary symptoms and the associated sexual dysfunction in patients with LUTS compared with tolterodine [9]. In these 2 studies, the recruited patients showed lower baseline IIEF compared with those in this current study, implying that mirabegron treatment may have a better treatment outcome on sexual function in patients with more severe ED. However, unlike previous studies, our results did not reveal an effect on erectile and ejaculatory functions. Although the ╬▓3-adrenoceptor agonist has been reported to facilitate smooth muscle relaxation in the resting filling phase in the penis in some studies [6,7], the ╬▓3 adrenoceptor agonist may not play a role during actual erection.
Although this present study was an RCT, it still had some limitations. The major limitation of this study was the small number of patients, especially those with different grades of ED. However, the current sample size is still enough to show the positive therapeutic effects of mirabegron on OAB symptoms and the lack of therapeutic effects on EF and ejaculatory function by both treatment approaches. The other limitation in the study was that there was no placebo to mirabegron and this was not one blind research. Another limitation of this research was that we could not offer a good explanation for the finding of a lack of improvement in EF in the combined behavioral therapy and mirabegron subgroup. We also acknowledge that prior reports of ED in mirabegron registry studies about male sexual function did not include large numbers of patients and a well-organized study design. Additional, multi-institutional RCTs with a larger number of participants, and different combination therapies, might be required to consolidate the possible effects of mirabegron on sexual parameters in patients with LUTS and OAB.
In summary, this research shows that both behavioral therapy alone and combination mirabegron and behavioral therapy improve male OAB symptoms but do not benefit EF and ejaculatory function. For male OAB, combination treatment achieved a greater improvement in OAB symptoms than behavioral therapy alone 4-week posttreatment. Future studies should prioritize determining the effect of mirabegron treatment on sexual function by combining different medications, which act on distinct signaling pathways related to penile erection.