INTRODUCTION
Patients with refractory lower urinary tract dysfunction (LUTD) caused by neurologic disorders exhibit upper urinary tract (UUT) deterioration involving upper urinary tract dilatation (UUTD) and serum creatinine (Scr) abnormalities due to lower bladder capacity and/or excessive intravesical pressure [1,2]. Augmentation uretero-enterocystoplasty (AUEC), a type of augmentation cystoplasty (AC) performed simultaneously with ureteroplasty and antireflux reimplantation, is an option for patients with UUT deterioration [3]. However, this procedure can involve complications [4], such as metabolic disturbances, urolithiasis, and even malignancy.
Botulinum toxin-A (BTX-A), produced from Clostridium botulinum, inhibits the release of acetylcholine, thereby suppressing contraction of the detrusor muscle [5]. Intravesical BTX-A injection therapy has been recommended as a second-line treatment for patients with neurogenic detrusor overactivity (NDO) [6]. Additionally, BTX-A detrusor injections increase bladder capacity, maintain low detrusor storage pressures, and control urinary incontinence [7]. Hence, the clinical application of BTX-A injection therapy can be further extended to the treatment of refractory LUTD given the following advantages: simple administration, minimal invasiveness, and lack of adverse events.
Currently, given the wide application of BTX-A injections, the number of patients choosing AUEC has significantly declined. However, little research has been conducted to evaluate the protective effect of BTX-A injections in patients with LUTD and UUT deterioration. The purpose of this cohort study was to determine the efficacy of BTX-A injection therapy in patients with UUT deterioration who had declined AUEC and to ascertain whether intravesical BTX-A injection therapy could serve as an alternative treatment to AUEC.
MATERIALS AND METHODS
This prospective comparative study was approved by the Ethics Committee of the China Rehabilitation Research Center (No. 2017-003-1). All patients with UUT deterioration who underwent AUEC or declined AUEC to receive BTX-A injections were included between January 2017 and December 2021.
All patient demographics and perioperative results were prospectively collected in our department. The patients who underwent intravesical BTX-A (Hengli; Lanzhou Biological Products, Lanzhou, China) injection therapy received serial 300-U injections at baseline and every 3–6 months thereafter. Patients were permitted to discontinue treatment if they were dissatisfied with the outcome or experienced intolerable adverse events. The AUEC procedures were performed by urological surgeons led by Professor Liao. All patients were treated with anticholinergics postoperatively and were evaluated every 3–6 months for therapeutic effects.
Inclusion and Exclusion Criteria
The indications for AUEC have been described in our previous studies [8–10]. The criteria for BTX-A injection therapy included patients who met the criteria for AUEC but declined AUEC. Urodynamic parameters, including maximum bladder capacity (MBC), maximum detrusor pressure (MDP), bladder compliance (BC), and vesicoureteral reflux (VUR), were assessed by video-urodynamic studies (VUDSs), and UUTD was evaluated using a magnetic resonance urography (MRU)-UUTD system [11,12]. Ultrasound does not reveal the kidney and ureter in the same image; thus, the MRU-UUTD system complemented the Society for Fetal Urology grading system in the identification of the entire urinary tract. Patients who declined to complete the follow-up or had previously undergone vesicoureteral reconstruction were excluded.
Statistical Analysis
All statistical analyses were performed using Empower R ( www.mpowerstats.com; X&Y Solutions, Inc., Boston, MA, USA). Continuous variables were expressed as the mean±standard deviation or median (interquartile range [IQR]) and evaluated using the Student t-test, 1-way analysis of variance, the Mann-Whitney U-test, or the Kruskal-Wallis H test. Categorical variables were presented as numbers (percentages) and evaluated with the chi-square or Fisher exact test. All statistical tests were 2-sided, with α=0.05.
General additive mixed models (GAMMs) with smooth curve fitting were used for analyzing repeated measurement data. A GAMM was used to assess the relationships between follow-up duration and MBC, MDP, BC, and Scr level, stratified by the 2 treatment protocols.
RESULTS
Patient Characteristics
In total, 121 consecutive patients were eligible for inclusion in the study, including 41 patients who received intravesical BTX-A injection therapy and 80 patients who underwent AUEC. The median follow-up duration was 17.0 months (IQR, 8.3–21.0 months) in the BTX-A group and 24.0 months (IQR, 6.50–26.00 months) in the AUEC group (P=0.21). The patient demographic characteristics are summarized in Table 1. Compared with patients who underwent AUEC, patients who received BTX-A injection therapy had a higher baseline MBC (152.0 mL vs. 86.0 mL, P<0.01) and were less willing to receive an invasive and irreversible procedure than the AUEC group.
Improvement in Urodynamic Parameters
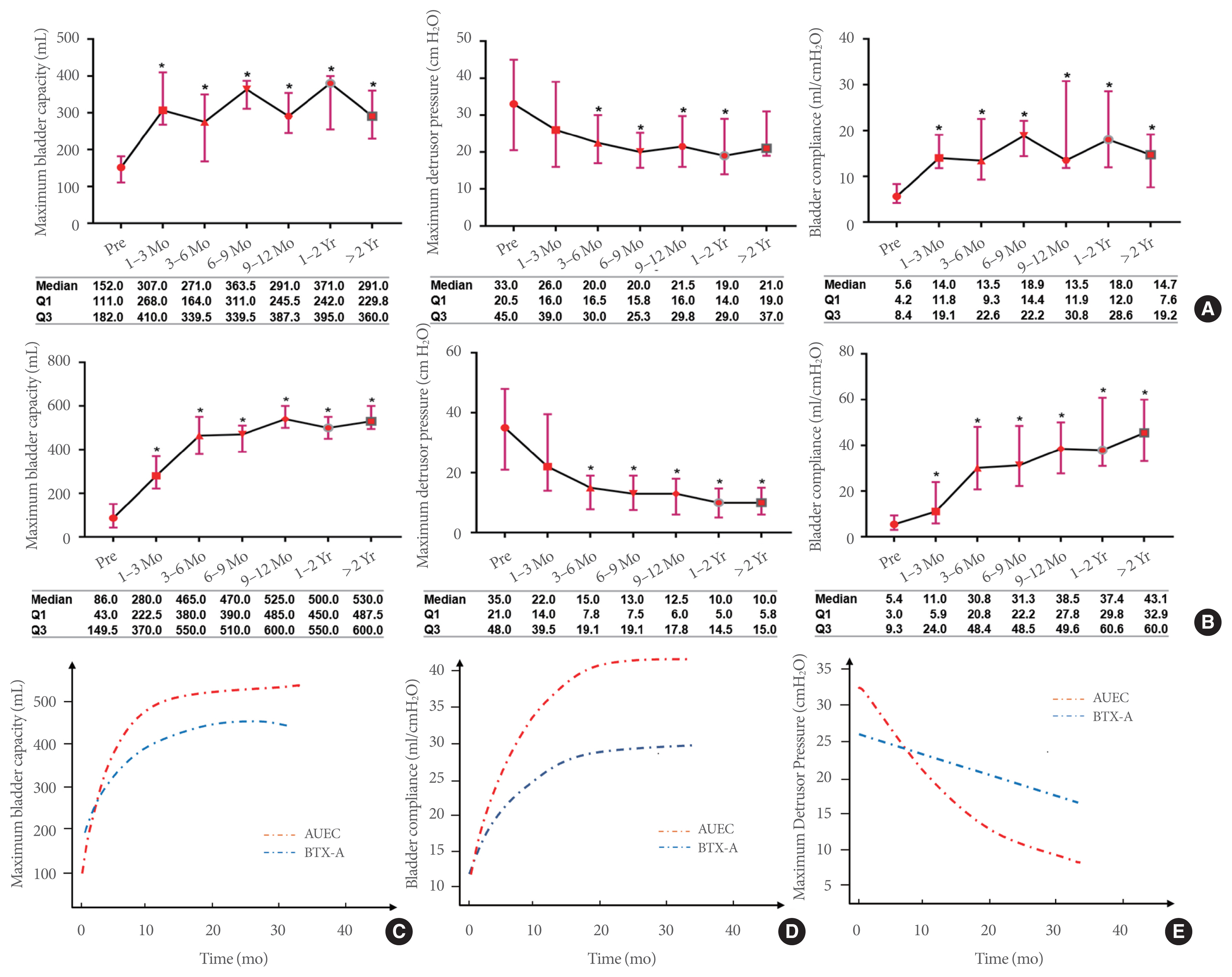
The VUDS outcomes in both groups showed a therapeutic effect on bladder function (Fig. 1). The continuous changes in urodynamic parameters seen in the follow-up evaluations of patients who received serial BTX-A injections are shown in Fig. 2A. Significant improvements in the MBC and BC were noted in the BTX-A group at the initial visit and every 3 months thereafter (all P<0.05). A declining trend in MDP was also noted 1–3 months after treatment compared to the pretreatment level, with a statistically significant difference after 3 months (P<0.05). Similarly, the MBC, MDP, and BC were significantly ameliorated by AUEC 1–3 months after surgery (P<0.05), and the improvements were sustained for >2 years (all P<0.05, Fig. 2B).
The GAMM with smooth curve fitting analyses showed differences in VUDS parameters between the BTX-A and AUEC groups during the follow-up period (Fig. 2C, D). The adjusted increase in MBC for the BTX-A and AUEC groups over 15 months was 13.62 and 22.67 (P<0.01), respectively, as shown in Table 2. A significant difference in the increased MBC was observed between the 2 groups (13.20, P<0.01). Similarly, the improvement in the BC in patients undergoing AUEC was greater 0–15 months after surgery than in the BTX-A injection group (2.82 vs. 1.09, P<0.01). Furthermore, the MBC and BC indices remained stable for patients in both groups at the 15-month follow-up. Interestingly, the MDP levels in both groups exhibited a time-dependent decrease (Fig. 2E), and a difference in the MDP reduction was seen between the BTX-A and AUEC groups throughout the follow-up period (−1.09, P<0.01).
Improvement in UUT Function
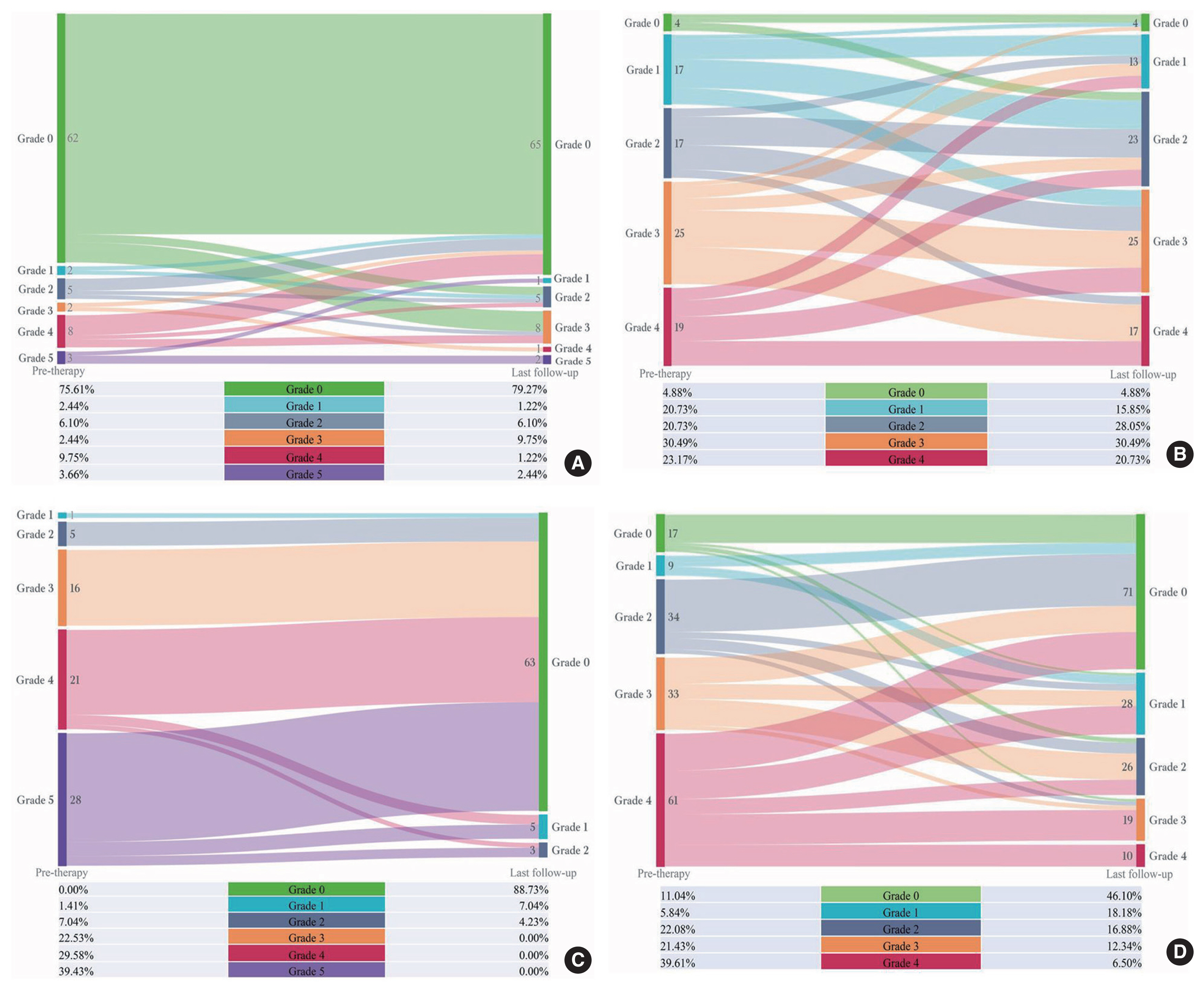
In the BTX-A group, a total of 82 ureters were analyzed. VUR was noted in 20 ureters, including 7 ureters with grade I–II VUR and 13 with grade III–V VUR. At the last follow-up evaluation, the VUR grade showed no improvement compared to baseline and the high-grade (≥III) VUR rate was unchanged (15.85% vs. 13.41%, P=0.66). The specific follow-up information is shown in Fig. 3A. In addition, UUTD was measured in 78 of 82 ureters in the BTX-A group. No improvements in UUTD were found when compared with baseline (Fig. 3B), and no reduction in the number of ureters with high-grade (≥III) UUTD was observed (53.66% vs. 51.22%, P=0.75). Eighty patients and 154 ureters were enrolled in the AUEC group, and there were 71 ureters (46.10%) with persistent VUR. A significant improvement in VUR was detected in the AUEC patients, and 63 of the 71 ureters (88.73%) with VUR resolved after AUEC treatment (Fig. 3C). A quantitative improvement in the MRU-UUTD grades was observed at the last follow-up (Fig. 3D); the rate of high-grade MRU-UUTD decreased from 61.04% to 18.84% (P<0.01).
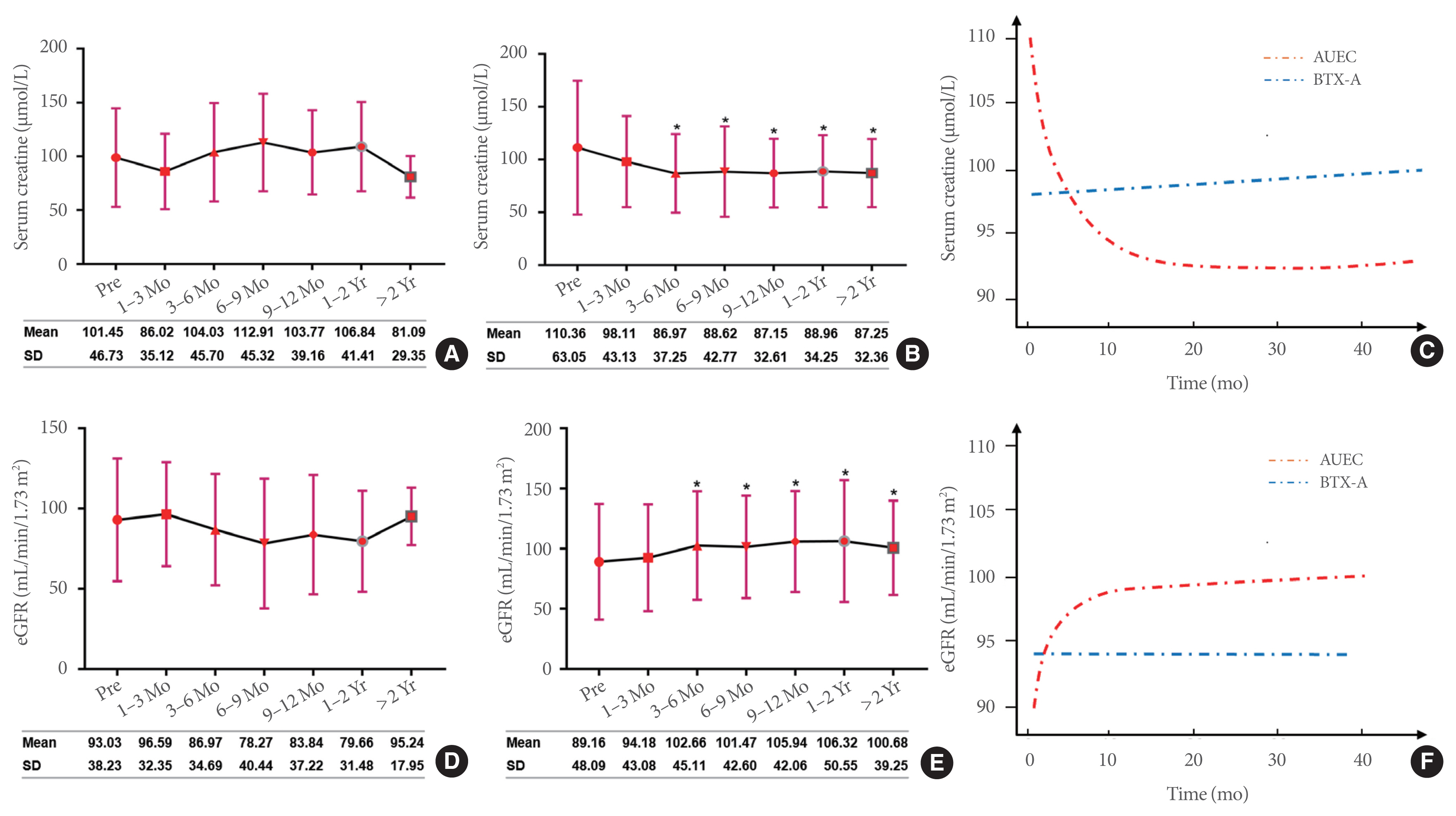
Renal function, represented by Scr levels, was analyzed as an important index of UUT deterioration, and the evolution of Scr levels over time was recorded for the 2 groups (Fig. 4A, B). Notably, no significant preoperative or postoperative difference was observed in the Scr levels of the BTX-A group (all P>0.05). The Scr level in patients who received AUEC significantly improved 3–6 months after surgery (110.36 μmol/L vs. 86.97 μmol/L, P<0.05), and this improvement was subsequently sustained. Reductions in the Scr level of the 2 groups were significantly different within the 15-month follow-up period (−1.36, P<0.01) (Table 2). The estimated glomerular filtration rates (eGFRs) calculated using the abbreviated Modification of Diet in Renal Disease formula, were opposite to the trend in Scr levels (Fig. 4D, E). Adjusted smooth curve fitting showed that the Scr and eGFR levels displayed marked improvements over time after patients underwent AUEC and remained stable during the postoperative follow-up (Fig. 4C, F). Conversely, in the BTX-A treatment group, no significant change was recorded in the Scr and eGFR levels over time compared with baseline, indicating stable renal function.
Complications
Some common complications occurred in the patients undergoing AUEC, including bowel dysfunction in 2 patients (Clavien-Dindo [CD] classification grade II), metabolic acidosis in 8 patients (CD grade II), and bladder calculus in 3 patients (CD grade IIIa); all problems were resolved by appropriate therapy. No apparent side effects or complications were observed in the BTX-A group during the follow-up evaluations. Finally, 11 patients with ineffective BTX-A outcomes were converted to AUEC for permanent correction.
DISCUSSION
Bladder management for neurogenic UUT deterioration should meet 3 main objectives: low-pressure urine storage, adequate urine drainage, and preservation of the UUT. AC is the mainstay for managing patients with LUTD in whom conservative measures have failed [13]. Previous studies have demonstrated that AC is a safe and effective procedure that can improve bladder function and quality of life parameters, thereby preserving renal function [9,10,14].
Compared with AC, AUEC is better able to protect UUT function for patients with VUR and UUTD with concomitant ureteral stenosis and tortuosity [3]. Because AC/AUEC is an open abdominal procedure involving the digestive and urinary systems, various complications may occur. The wide-ranging application of minimally invasive techniques such as intravesical BTX-A injection therapy in the management of LUTD has led to a sharp decline in the application of AC/AUEC [15]. Previous studies have shown that intradetrusor BTX-A injections improve urgency incontinence episodes and quality of life [5,16]. Theoretically, the detrusor injection of BTX-A improves urodynamic parameters by inhibiting the efferent and afferent pathways [2], which has been demonstrated in cases of poor BC and NDO [17,18]. We compared the therapeutic effects of BTX-A injection therapy and AUEC for patients with UUT impairment. Our results showed that the VUDS parameters after BTX-A injections improved significantly, and were consistent with the results of previous studies [19,20]. The intravesical filling pressure decreased significantly, suggesting that BTX-A injection therapy can establish a compliant bladder with reduced bladder pressure and increased bladder capacity to avoid renal compromise and UUT deterioration. However, because BTX-A produces a temporary (3–6 months) and reversible denervation [21], the potency of the muscle relaxant effect on the detrusor muscle is inadequate and short-lived. Although the smoothing analysis curves for the VUDS parameters revealed that both treatments had a profound impact on improving bladder function, those who underwent AUEC had a significantly greater improvement in MBC, MDP, and BC than patients who received BTX-A injection therapy.
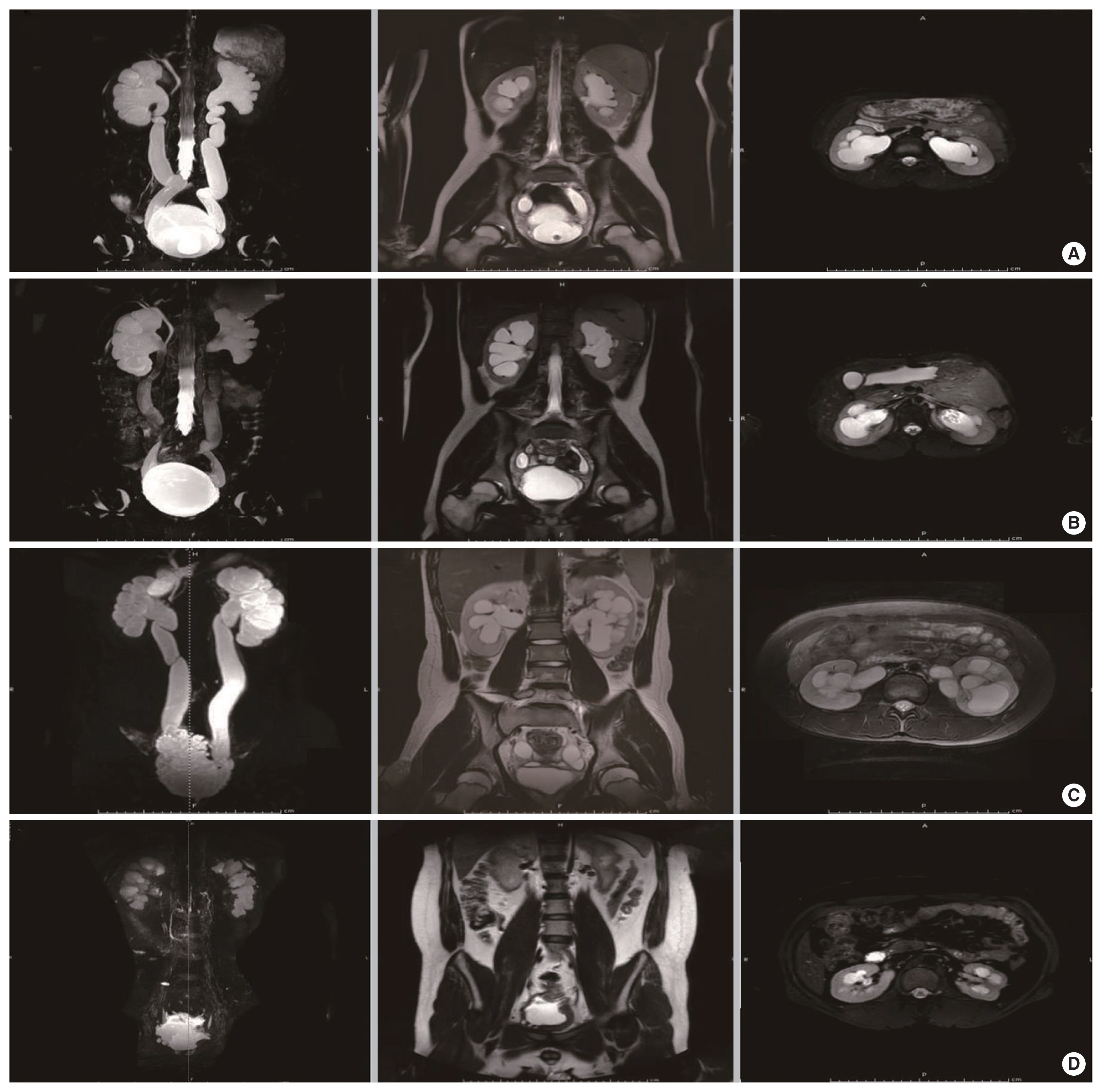
In addition to improved bladder function, improvements in VUR and UUTD are important indicators in the evaluation of both treatment regimens. The protective role of AC/AUEC for UUT in LUTD patients has been recognized [3,8–10]. Experts have argued that intradetrusor BTX-A injections not only make the bladder compliant and help avoid renal compromise and UUTD [22], but have also resulted in significant improvements in VUR [23] and decreased the risk of UUT damage [24]. Our data revealed that, although BTX-A injection therapy can improve bladder function, decrease VUR and UUTD, and prevent renal function deterioration, it remained unsatisfactory and the MRU-UUTD grade distribution was not substantially altered in the last follow-up evaluation. Therefore, this treatment demonstrated little improvement in the renal function of patients with UUT deterioration. We propose that the following factors may account for the unsatisfactory therapeutic effect: First, the urodynamic parameters of BTX-A injection therapy showed less favorable outcomes than AUEC, and the improvements in bladder capacity and pressure were insufficient (maintained around 20 cm H2O) after BTX-A injection therapy. Therefore, we concluded that BTX-A injections only eliminated high-pressure VUR and had little effect on low-pressure VUR (Fig. 1A, B) and UUTD (Fig. 5A, B). Second, BTX-A injections minimally affect detrusor muscle relaxation and have a short duration of action, which impairs the ability to establish an elastic low-pressure reservoir to relieve UUTD. In addition, UUTD is often found with concomitant ureteral stenosis and tortuosity, particularly in patients with advanced-stage neurogenic bladder and with a longer disease duration. BTX-A injection therapy could not correct ureteral stenosis/obstruction and tortuosity above the bladder. Third, because medical developments are uneven across China, bladder wall fibrosis induced by a long history of illness and inappropriate bladder management can disrupt antireflux mechanisms in the ureterovesical junction. Thus, BTX-A injection therapy ameliorates bladder capacity but cannot reconstruct the antireflux mechanism. In contrast, the antireflux reconstruction and ameliorated bladder parameters achieved by AUEC dramatically reduced the postoperative occurrence of VUR (Fig. 1C, D). Importantly, ureteral obstruction and tortuosity can be completely relieved by AUEC through ureterolysis and tailoring to release adhesive bands, straighten tortuous positions, and shorten superfluous ureters. This method ensured unobstructed drainage of urine from the kidneys and improved renal function in patients with LUTD (Fig. 5C, D) [3].
Although BTX-A injection therapy is a less invasive and lower-cost option [25], the treatment requires repeated injections at 6-month intervals to maintain the initial favorable therapeutic effect. In this study, patient follow-up and adherence to treatment were not as high as we had expected. Moreover, the quality of life in the AUEC group was superior to that of the BTX-A group [26], possibly because of the long-term effectiveness of AUEC when compared to intermittent BTX-A injection therapy. Notably, the cost-effectiveness of AUEC gradually emerged as the cost of BTX-A injections increased and the complication rate of AUEC decreased [25]. Ultimately, 11 patients with unsatisfactory outcomes following BTX-A injections were converted to permanent correction with AUEC.
This was the first study to explore the protective effects of BTX-A injection therapy on the UUT and compare the outcomes to AUEC outcomes. In addition, we were the first to objectively report that BTX-A injection therapy failed to alleviate UUT impairment and protect UUT function in all patients with LUTD, especially those with ureteral tortuosity and obstruction that could be improved by AUEC. The main limitation of this prospective, single-center study was the lack of randomization between the 2 patient groups. Due to technology and cost limitations, most patients did not undergo an isotope renogram and cystatin C to evaluate differences in renal function, and Scr levels did not fully reflect renal function. Finally, data from the present comparative study should be validated externally, preferably by multicenter experiences.
In conclusion, minimally invasive intradetrusor BTX-A injection therapy was used to manage LUTD, and was shown to provide urodynamic benefits, including increased bladder capacity and decreased storage pressure. However, therapeutic relief of VUR and UUTD, and improved renal function remained unsatisfactory, particularly in patients with advanced LUTD and longer disease duration. Our data confirmed that AUEC generated greater improvement in urodynamic parameters and UUT function than serial BTX-A injections. Therefore, we believe that intravesical BTX-A injection therapy should not serve as an alternative protocol for AUEC. Although the application of AUEC has been declining in the treatment of LUTD, it still plays an important role for patients with refractory, advanced-stage LUTD.