Effect of Nerve-Sparing Radical Prostatectomy on Urinary Continence in Patients With Preoperative Erectile Dysfunction
Article information

Abstract
Purpose:
We aimed to assess whether nerve-sparing radical prostatectomy (nsRP) is associated with improved recovery of urinary continence compared to non–nerve-sparing radical prostatectomy (nnsRP) in patients with localized prostate cancer and preoperative erectile dysfunction.
Methods:
A total of 360 patients with organ-confined prostate cancer and an International Index of Erectile Function score of less than 17 were treated with nsRP or nnsRP in Seoul St. Mary’s Hospital. Patients who received neoadjuvant or adjuvant androgen deprivation therapy or had a history of prostate-related surgery were excluded. Recovery of urinary continence was assessed at 0, 1, 3, 6, and 12 months. Postoperative recovery of continence was defined as zero pad usage. The association between nerve-sparing status and urinary continence was assessed by using univariate and multivariate Cox regression analyses after controlling for known predictive factors.
Results:
Urinary continence recovered in 279 patients (77.5%) within the mean follow-up period of 22.5 months (range, 6–123 months). Recovery of urinary continence was reported in 74.6% and 86.4% of patients after nnsRP and nsRP, respectively, at 12 months (P=0.022). All groups had comparable perioperative criteria and had no significant preoperative morbidities. Age, American Society of Anesthesiologists score, and nerve-sparing status were significantly associated with recovery of urinary continence on univariate analysis. On multivariate analysis, age (hazard ratio [HR], 1.254; 95% confidence interval [CI], 1.002–1.478; P=0.026) and nerve-sparing status (HR, 0.713; 95% CI, 0.548–0.929; P=0.012) were independently associated with recovery of urinary continence.
Conclusions:
nsRP, as compared to nnsRP, improves recovery rates of urinary incontinence and decreases surgical morbidity without compromising pathologic outcomes.
INTRODUCTION
Prostate cancer is one of the most common cancers worldwide. In Korea, the incidence of prostate cancer increased from 8.4 per 100,000 population in 1999 to 27.4 per 100,000 in 2011. This increase is the second highest among cancers affecting men. Conversely, 5-year relative survival rates have improved from 55.9% in patients diagnosed from 1993 to 1995 to 92.0% in those diagnosed from 2007 to 2011 [1]. With increasing survival rates, quality of life issues have become important concerns for patients undergoing radical treatment of prostate cancer, as well as for their physicians. Radical prostatectomy is therefore assessed based on functional outcomes, which include urinary incontinence and erectile dysfunction, in addition to oncologic outcomes.
Several surgical techniques have been described for achieving recovery of urinary continence after radical prostatectomy [2-4]. However, a recent meta-analysis has identified posterior reconstruction with or without anterior reconstruction as the only procedure that enabled significant early recovery of urinary continence [5]. The role of nerve-sparing approach in enabling early recovery of urinary continence remains controversial [6-9]. Inclusion of patient groups with variable degrees of preoperative erectile function could have possibly contributed to the limitations of prior studies in addressing this controversy. Therefore, this study was designed to assess whether nerve-sparing radical prostatectomy (nsRP) enabled recovery of urinary continence as compared to non–nerve-sparing radical prostatectomy (nnsRP) in patients with localized prostate cancer and preoperative erectile dysfunction.
MATERIALS AND METHODS
A total of 360 patients who underwent radical prostatectomy between January 2003 and December 2012 and meeting the following criteria were included: (1) organ-confined prostate cancer, (2) preoperative erectile dysfunction (International Index of Erectile Function-5 [IIEF-5] score <17), (3) no neoadjuvant or adjuvant androgen deprivation therapy or radiation therapy, (4) no previous prostate-related surgery, (5) a follow-up duration of over 1 year. After approval from the Institutional Review Board at the Catholic University of Korea, Seoul St. Mary’s Hospital (approval number: KC14RISI0934), clinical data of eligible patients were extracted from the Smart Prostate Cancer database of Seoul St. Mary’s Hospital [10]. Extracted data included age, body mass index, American Society of Anesthesiologists (ASA) score, preoperative prostate-specific antigen (PSA) level, clinical stage, biopsy Gleason score, and pathologic outcomes. Preoperative lower urinary tract symptoms and erectile function were assessed before surgery by using the International Prostate Symptom Score (IPSS) and IIEF-5 questionnaires, respectively.
Radical prostatectomy was performed by using a laparoscopic (n=275, 76.4%) or robotic (n=85, 23.6%) approach. Nerve-sparing prostatectomy was performed by using the interfascial technique described by Gaston and colleagues [11], and was selected by each physician, independent of preoperative erectile function. Recovery of urinary continence was assessed at 1, 3, 6, and 12 months postoperatively and every 3–6 months thereafter. Postoperative recovery of urinary continence was defined as zero pad usage.
IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA) was used for analysis. Data was compared by using Mann-Whitney U-test for continuous variables and chi-square test for categorical variables. Kaplan-Meier analysis assessed time to recovery of urinary continence according to nerve-sparing status. The association between nerve-sparing status and urinary continence was assessed by using univariate and multivariate Cox regression analyses, after controlling for known predictive factors.
RESULTS
All baseline parameters, except preoperative IIEF-5 score and preoperative serum PSA level, were comparable between the two groups (Table 1). The mean operative times for the nsRP and nnsRP groups were 199.7 and 206.5 minutes, respectively (P=0.044). The mean estimated blood loss was 391.1 mL in the nsRP group and 415.3 mL in the nnsRP group respectively (P=0.489) (Table 2). The nnsRP group had a significantly higher perioperative complication rate than the nsRP group (2.0% vs. 17.0%, P=0.003). However, complications were mostly less than grade III. Table 2 shows the pathologic outcomes of both the nsRP and nnsRP groups. There were no significant differences in pathologic T stage, pathologic Gleason score, and positive surgical margins between the nsRP and nnsRP groups.

Patient demographics and baseline data
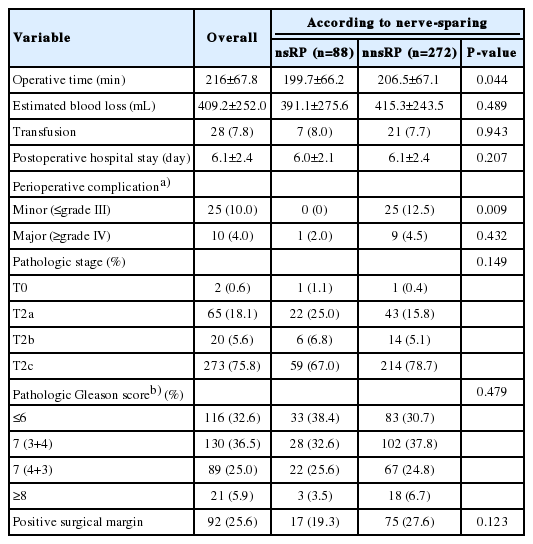
Perioperative and pathologic outcomes
At the mean follow-up of 22.5 months (range, 6–123 months), urinary continence recovery was noted in 279 patients (77.5%). Urinary continence recovery rates at 3, 6, and 12 months were 33.8%, 58.3%, and 77.6% in the nnsRP group and 54.5%, 72.7%, and 85.2% in the nsRP group, respectively (Fig. 1, log-rank test, P=0.003). When patients were stratified according to age (≤70 yr vs. >70 yr), the benefits of nsRP in enabling better urinary continence recovery rates reached statistical significance in older patients (nnsRP vs. nsRP; 69.0% vs. 95.0%, P=0.014), but not in younger patients (79.5% vs. 83.8%, P=0.576).

Urinary continence recovery rates in nsRP and nnsRP (P=0.003). nsRP, nerve-sparing radical prostatectomy; nnsRP, non–nerve-sparing radical prostatectomy.
Table 3 shows univariate and multivariate Cox regression analyses for predicting recovery of urinary continence. On univariate analysis, age>70 years, ASA score, total IPSS score, and nerve-sparing status were significantly associated with recovery of urinary continence. On multivariate analysis, age>70 years (hazard ratio [HR], 1.254; 95% confidence interval [CI], 1.002–1.478; P=0.026) and nerve-sparing status (HR, 0.713; 95% CI, 0.548–0.929; P=0.012) were independently associated with recovery of urinary continence (Table 3).
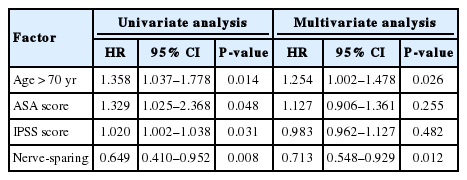
Univariate and multivariate Cox proportional hazard regression analyses for predicting recovery of urinary continence after radical prostatectomy
DISCUSSION
The primary challenge in radical prostatectomy for prostate cancer, as currently recognized, is improvement in the quality of life. Urinary incontinence and erectile dysfunction are among the factors that affect the quality of life in these patients. Although there are several studies on factors predicting early recovery of urinary continence after radical prostatectomy, their results are conflicting about the impact of a nerve-sparing approach on such recovery [6-9,12]. In our study, which compared nnsRP and nsRP in patients with preoperative erectile dysfunction, patients undergoing nsRP demonstrated significantly better rates of recovery of urinary continence. When adjusted for age, the difference between nnsRP and nsRP was statistically significant for older patients (>70 years) alone. Further, in our study, patients treated with nsRP had a 28.7% reduction in urinary incontinence after adjusting for factors known to be clinically significant for recovery of continence.
Despite the importance of nerve-sparing procedure, many urologists do not choose to perform nsRP in patients with preoperative erectile dysfunction, older age, or advanced disease. Stember et al. [13] defined factors related to nnsRP use as baseline erectile function, biopsy Gleason sum, clinical stage≥T2, patient age, and percentage of positive biopsy cores. They demonstrated that patients were one and half (1.5) times more likely to undergo nsRP with every one point increase in the erectile function score. Decisions of patients yield a similar conclusion. Lavery et al. [14] reported that 64% of patients with moderate-to-severe erectile dysfunction prefers nnsRP.
Previous studies have shown significant [6,7,15-18] or no association [8,9] between nsRP and improved recovery of urinary continence. Kundu et al. [8] demonstrated that the recovery of urinary continence was associated with younger age but not with nerve-sparing surgery. Similarly, Tzou et al. [9] reported that attempted or successful nsRP did not result in better rates of urinary continence. However, other studies have reported that attempted or successful nerve-sparing was a statistically significant predictor for recovery of urinary continence when accounting for all other factors by multivariate analysis [6,7,15]. A recent systematic review and meta-analysis by Reeves et al. [18] supported the importance of nsRP in enabling early recovery of urinary continence. The meta-analysis demonstrated that nsRP, compared to nnsRP, had significantly better early but not long-term continence recovery. Risk ratios were 1.48 (range, 1.34–1.63; P<0.001) at ≤6 weeks, 1.24 (range, 1.09–1.42; P=0.001) at 3–4 months, and 1.20 (range, 1.04–1.39; P=0.02) at 6 months, respectively. No significant difference was observed in rates of urinary continence after nsRP and nnsRP at 12 or 24 months. Despite the systematic approach of this review, the significant risk of bias of individual studies diminishes the evidence provided to support the use of nsRP for improved recovery of urinary continence in patients with preoperative erectile dysfunction.
The role of nerve-sparing in patients with preoperative erectile dysfunction is yet to be clarified. Recent studies have demonstrated that nsRP in this population may have advantages beyond improving erectile function [17,16]. Khoder et al. [16] treated a total of 420 impotent prostate cancer patients with bilateral intrafascial or interfascial nsRP and found higher continence recovery rates with nerve-sparing procedures. The best results were achieved in the intrafascial nsRP group. Similarly, Harris et al. [17] demonstrated that nerve-sparing improved postoperative urinary but not sexual function in men with low baseline sexual function. All these previous studies suggest that men with preoperative erectile dysfunction may also benefit from nerve-sparing procedures.
Nerve-sparing is important for recovery of urinary continence and this recovery may be based on several proposed mechanisms. First, membranous urethral microcirculation may be a critical part of the continence mechanism. John et al. [19] investigated the results of endoscopic urethral tissue blood flow before and after radical prostatectomy in 37 continent patients. They found that membranous urethral blood flow significantly decreased after radical prostatectomy from 18.8 to 11.9 mL/min/100 g of tissue. Patients undergoing nsRP may, therefore, have better pelvic vascular status and more preserved membranous urethral vascular integrity than those undergoing nnsRP. This may contribute to improved recovery of urinary continence after nsRP. Second, there is evidence associating cavernous nerve injury with impaired membranous urethral sensitivity. John et al. [20] found that posterior urethral sensitivity and pressure transmission were impaired immediately after prostatectomy, and improvement in these parameters after 6 months was associated with the restoration of continence. Catarin et al. [21] prospectively identified alterations in the pelvic and membranous urethral afferent and efferent innervation after nsRP by using several neurophysiological tests as well as a validated questionnaire. Sensory and motor pudendal innervation was unaffected after surgery, whereas autonomic afferent denervation of the membranous urethral mucosa was found in 77.3% of patients. There was significant prevalence of autonomic afferent denervation in patients with occasional leakage of urine (91.7%).
Improved quality of life and decreased surgical morbidity are critical elements in the decision to choose a nerve-sparing procedure, especially in older patients. This study demonstrates that the benefits of nsRP in terms of improvement in recovery of urinary continence is significant in older (>70 years) rather than younger patients (≤70 years). Khoder et al. [16] demonstrated that older patients (>70 years) had a higher rate of full continence with nsRP (80%) compared to nnsRP (65%) and this difference tended towards significance (P=0.052). The reason for this difference based on age may be owing to excellent continence outcomes in the younger age group independent of nerve-sparing procedure. Perioperative complication rates and operative time were significantly lower in the nsRP group than the nnsRP group in our study. A previous study comparing nerve-sparing and wide-excision groups similarly showed a significant difference in operative time (65 and 70 minutes, respectively, P<0.001) and blood loss (150 mL and 200 mL, respectively, P<0.001) between the 2 groups [16]. The advantages observed by us should encourage surgeons to perform nsRP more frequently to improve quality of life and minimize surgical morbidity, even in older patients with preoperative erectile dysfunction.
In conclusion, our study involving patients with localized prostate cancer and preoperative erectile dysfunction provides evidence supporting the role of nsRP in enabling improved recovery rates of urinary continence. Additionally, nsRP was found to decrease surgical morbidity when compared to nnsRP, without compromising pathologic outcomes. Based on our study, we recommend surgeons to consider nsRP whenever oncologically and technically feasible irrespective of patients’ age or status of erectile dysfunction.
Notes
Grant Support
This study was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HI14C1203).
Research Ethics
After approval from the Institutional Review Board at the Catholic University of Korea, Seoul St. Mary’s Hospital (approval number: KC14RISI0934), clinical data of eligible patients were extracted from the Smart Prostate Cancer database of Seoul St. Mary’s Hospital.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.