Epidermoid cyst in the kidney occurs very rarely and only a few cases have been reported in the literature [1-6]. Although it is a very uncommon lesion, a calcified intrarenal lesion has to be suggested as an important landmark for differential diagnosis of renal epidermoid cyst [3]. Because the epidermoid cyst is benign, renal preservation surgery can be an appropriate management if a prompt diagnosis is preoperatively made [6]. However, a noncalcified soft tissue mass in the renal pelvis is highly suggestive of urothelial carcinoma, nephroureterectomy should be basically considered. It has been discussed that the epidermal remnant of Wolffian duct, squamous metaplasia after chronic irritation with urinary stone [2,3,6], and traumatic implantation [2,6] are possible cause of a renal epidermoid cyst. The transitional epithelium, known as urothelium, is a distinctive structure covering in the urinary tract. Uroplakins consists of apical urothelial membrane and are considered to be a biochemical marker of urothelial differentiation [7]. Is there any cellular basis of urothelial squamous metaplasia in the development of epidermoid cyst in the renal pelvis? It is not clear what the role of uroplakins in the squamous metaplastic lesion. Herein, we report an atypical case of an epidermoid cyst in the renal pelvis with an emphasis on its histogenetic origin using immunohistochemistry.
CASE REPORT
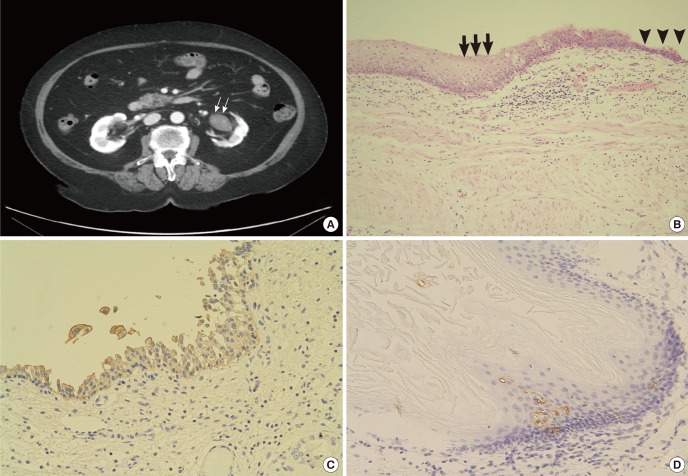
A 73-year-old female was admitted for surgical removal of a left renal pelvic mass. She has taken antihypertensive agents for 30 years and received percutaneous coronary intervention due to stable angina 3 years ago. During routine follow-up, a renal mass was incidentally detected 2 months ago. She denied any episodes of renal colic or urolithiasis. On physical examination, there was no tenderness on the area of costovertebral angle. Laboratory values revealed a marginal elevation of serum creatinine (1.21 mg/dL). Urinalysis and urine cytology showed no evidence of inflammation or malignant cells. The ultrasonography showed an echogenic mass within the renal pelvis and mild dilation of several calyces. The calcified lesion was not found on plain radiograph of the abdomen (kidneys, ureters, and bladder). An abdominopelvic computed tomography revealed a noncalcified soft tissue mass in the left renal pelvis on precontrast enhancement scan. It showed slight enhancement after contrast administration (Fig. 1A). The preoperative radiologic diagnosis was favored as a urothelial carcinoma of the renal pelvis. A conventional left nephroureterectomy was performed.
The cut surface of the resected specimen revealed a 5×3×2 cm-sized, well-defined ovoid, cystic mass which was compactly filled with white and reddish tan-colored amorphous materials in the pelvis. Histologically, the cystic lumen contained multiple keratinous materials and much of the cystic lining epithelia were denuded. The remaining portion was lined with hyperplastic urothelium and keratinizing squamous epithelium (Fig. 1B). These two epithelial areas were sharply demarcated from each other. Immunohistochemical staining using antibodies against uroplakin II (1:100; Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA) and cytokeratin 7 (CK7) (1:100; Dako, Glostrup, Denmark) was performed to identify epithelium-specificdifferentiation. The cells lining urothelia were strikingly positive for uroplakin II (Fig. 1C) and CK7. In contrast, most of the cells in the lining of squamous epithelia were negative for these urothelial specific antibodies. However, some portion of the squamous epithelia interestingly contained a few uroplakin-positive cells (Fig. 1D) and some more CK7-positive cells.
DISCUSSION
Even though the epidermoid cyst of the kidney is a very rare to be characterized, the typical features of the lesion can be summarized as follows. The clinical symptoms are flank pain, gross hematuria, or lower urinary tract symptoms. The epidermoid cysts are usually found as an intrarenal lesion [1,2,4,5]. The calcified inhomogeneous lesion, combined renal stone, and previous renal surgery are other important clinical clues for the renal epidermoid cyst (Table 1). To date, two cases of epidermoid cyst in the renal pelvis have been reported. They also showed a typical calcified lesion combined with renal stone like other renal epidermoid cysts [3,6]. With these reasons, it seemed hard to think of epidermoid cyst as a presumptive diagnosis before surgery in this case. To the best of our knowledge, this case of a noncalcified epidermoid cyst in the renal pelvis is the first report in the English literature.
The histology of a typical epidermal cyst that was lined by stratified squamous cells with laminated keratins. Although epidermoid cyst of the skin is a common lesion resulted from implantation of epidermis into the dermis, histogenesis of epidermoid cyst in the kidney remains uncertain. As a possible histogenetic mechanism, either epidermal embryonic remnants of Wolffian ducts or traumatic implantation of transformed epithelial cells during renal operation have been proposed. The extension of squamous metaplastic changes from the upper ureter to the pelvocalyceal system in prolonged irritative condition induced mostly by stones is considered as the other plausible explanation [2,3,6]. However, the cellular basis of squamous metaplasia is not fully understood in this rare condition.
The urothelium forms an extraordinarily effective permeability barrier. To perform these functions, the apical surface of urothelium is highly specialized as it is covered almost by urothelial plaques which are composed of uroplakins [7]. Four uroplakins (Ia, Ib, II, and III) have been isolated and are considered to be biochemical markers of terminal urothelial differentiation. CK7 is an intermediate filament proteins expressed in a wide variety of simple epithelia but not in the squamous epithelia. Normal urothelium and urothelial tumors express CK7 in a significant percentage of cases [8]. Therefore, CK 7 is also considered to be a marker of urothelial differentiation.
It is well known that vitamin A deficiency can induce keratinizing squamous metaplasia in a variety of epithelia including urothelium [9]. Recently, the heterogeneity in urothelial metaplasia has been reported [7]. The urothelial keratinization in the vitamin A-deficient mice bladder occurred heterogeneously adjacent to areas lined with normal appearing urothelium. The sharp boundary between the keratinized epithelium and the seemingly normal urothelium was maintained with no intermediated cells. According to the our histologic examination, nearly almost of the urothelial cells in the cystic lining were positively stained against both uroplakin II and CK7, but most of the squamous epithelial cells were negative for these antibodies. The two epithelia were sharply delineated and more distinctly distinguishable in the immunohistochemical stained sections. These features were similar with heterogenous metaplasia of the animal urothelium in the previous study [7]. However, some squamous epithelia contained a few uroplakin-positive cells and CK7-positive cells to some extent. Even though the significance of few uroplakin expressions in squmous epithelium should be evaluated by other studies, is this an indirect evidence of the direct transformation of umbrella cells to squamous metaplasia or dedifferenctiation of metaplastic squamous epithelium to urothelium?