Posterior urethral valves (PUV) are now most frequently suspected by antenatal ultrasound. Postnatally, PUV can have a broad spectrum of presentation ranging from a life threatening pulmonary hypoplasia due to oligohydramnios, to milder obstruction with few pathological signs or symptoms that may escape early detection and manifest only in later childhood, adolescence or even adulthood [1-4]. Older patients usually present with lower urinary tract symptoms (LUTS), overflow incontinence, recurrent infections, or less commonly, ejaculatory dysfunction, gross haematuria and renal insufficiency [3,4]. We present the rare case of an adolescent who presented late with overflow urinary incontinence and preserved renal function.
CASE REPORT
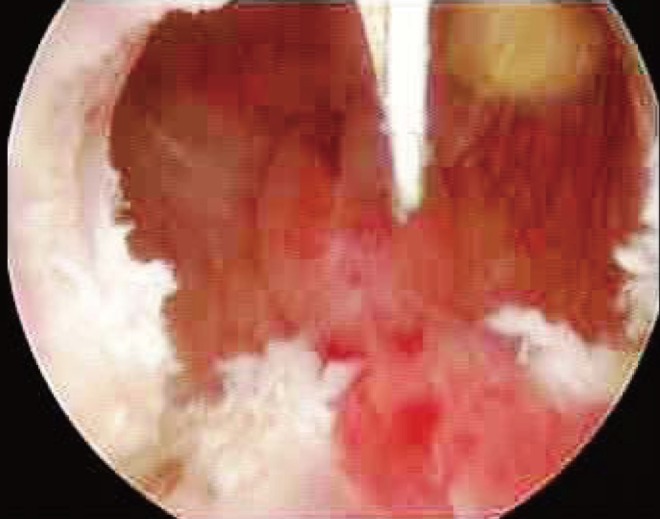
An 18-year-old male presented to us with a 1-year history of continuous dribbling of urine both during day and night. He also complained of poor stream of urine with associated straining to void, frequency, nocturia and sense of incomplete evacuation of urine. He claimed to have been voiding "normally" throughout childhood. He did not have any history suggestive of urinary tract infections. His past medical history was insignificant. The patient's abdominal exam revealed palpable urinary bladder. Neurologic exam and lumbrosacral spine were normal. Serum chemistries were normal with urea of 25.7 mg/dL and creatinine of 1 mg/dL. Urine studies were unremarkable. Abdominal Ultrasound showed a grossly distended and thick-walled bladder, with high post void residue. No spinal abnormalities were seen on kidney, ureter, and bladder X-ray. A voiding cystourethrogram was performed, which showed a pear shaped bladder with irregular outline and thickening with a dilated posterior urethra (Fig. 1). Urethrocystoscopy with 17 Fr., 30°, rigid cystoscope showed a classic image of type 1 PUV (Fig. 2); the leaflets were thick, fibrous which were incised at the 5, 7 and 12 o'clock positions using a Collins Knife on a working element (Figs. 3, 4). Severe bladder trabeculations were seen. The Foley catheter was removed the next day and he was voiding with a maximal flow of 20 mL/sec, average flow of 8 mL/sec and 170 mL voided volume with a regular curve on uroflowmetry. He was discharged and on follow-up at 6 weeks had improved symptomatically with better flow rates and minimal post void residue. Postvalve ablation ultrasound demonstrated minimal residual volume.
DISCUSSION
Prior to the widespread use of antenatal ultrasound, late presentation of PUV was considered a good prognostic sign, suggestive of lesser degrees of obstruction [3]. Late presentations are rare nowadays, but scattered cases have been reported in the past two decades [1,3,4]. Late presenting PUV patients may display both bladder storage and emptying symptoms, incontinence, sexual dysfunction and recurrent urinary tract infections [1,3,4]. In one of the earliest and largest adult series, Mahony and Laferte [4] studied 26 cases of PUV in men over 21 years of age. The most common presentation was frequency and urgency, followed by obstructive voiding symptoms predominantly in men older than 40 years. Similar series have also found that obstructive symptoms and incontinence predominate in patients with late PUV presentation [3,5]. Lower urinary tract dysfunction is a commom finding in boys after PUV ablation, regardless of age at presentation.
Thirty-eight to 70% of neonatally diagnosed and treated PUV patients develop the "valve bladder syndrome," which represents the spectrum of bladder dysfunction that manifests many years after definitive treatment of valves [6]. De Gennaro et al. [6] have shown the progressive natural history of urodynamic patterns in 30 boys treated for PUV. Bladder dysfunction was present in 70%, and changed from unstable/hypercontractile in infancy, to hypocontractile in childhood, to a true myogenic failure in adolescence, despite early valve ablation. Holmdahl et al. [7] suggested that these 3 urodynamic findings are variations of the same basic pattern evolving with time toward decompensation in early presenters, despite early correction of obstruction. Ziylan et al. [5] compared the natural history of both early and late presenters, and showed that bladder dysfunction was present in 85% of the late presenters (mean age, 8.8 years); however, the same characteristics of dysfunction were also found in patients with early diagnosis (mean age, 17.7 months). This similar pattern of progressive bladder dysfunction may indicate a common pathophysiology for both early and late presenters. Indeed, some suggest that the outlet obstruction during intrauterine development causes permanent changes in detrusor structure, which may be responsible for the bladder deterioration observed in adolescence [5,8]. End-stage renal disease (ESRD) can occur in up to 43% of patients with PUV by age 30 [9]. A review by Bomalaski et al. [1] on 47 patients aged 5 to 35 years with delayed-presentation of PUV revealed that, at diagnosis, renal insufficiency was present in 35% and ESRD in 10%. Indeed, although some suggest that late-presenting PUV carries a better long-term prognosis, renal impairment can occur at any age.
Overall, long-term outcomes after valve ablation in late presenters are variable. In their series (mean follow-up, 32 months), Bomalaski et al. [1] found that incontinence, dysuria and weak urinary stream resolved in 18% and improved in 45%, while renal function worsened in 10%. In Schober's review of 70 late-presenting PUV patients (mean age, 7 years; range, 2 to 14 years), 68% had good or improved bladder emptying immediately after valve ablation; however, 63% had ongoing daytime urinary incontinence, nocturnal enuresis or urinary frequency at mean follow-up of 25 months [3]. Eighty percentage of the patients with hydronephrosis at presentation showed no significant improvement after valve ablation. In such cases, aggressive management with clean intermittent catheterization and overnight bladder drainage should be promptly initiated to prevent upper urinary tract damage. Rapid improvement is usually seen, as reported in recent studies [9,10]. Also, we plan to follow the case for a late developing renal insufficiency.
Our case highlights the late presentation of PUV with preserved upper urinary tracts. As outlined, bladder dysfunction even in neonatally treated boys seems to evolve with age. The non-evolution towards decompensation of our patient's bladder until age 18 will remain unclear, but we suspect that it was arrested at the early stages of hypertrophy. This unusual case underscores the spectrum of clinical findings associated with late-presenting valves. It adds to the small, but growing, body of literature on delayed PUV presentation and emphasizes the importance of a high degree of clinical suspicion when evaluating boys of any age with LUTS and unusual urologic complaints.