Sex Differences in Lower Urinary Tract Symptoms in Older Korean Adults Living in Rural Areas: Prevalence, Quality of Life, and Associated Factors
Article information

Abstract
Purpose
Urinary incontinence (UI) is associated with nursing home admission, functional decline, and risk of death among community-dwelling older adults. Little information, however, is available on sex differences in lower urinary tract symptoms (LUTS) in older Korean adults exclusively living in rural areas. This study examined sex-related differences in LUTS, factors associated with UI in older adults living in rural areas, and health-related quality of life (HRQoL) in incontinent older adults.
Methods
This was a cross-sectional study in which face-to-face interviews were conducted at 15 rural community-health centres. A total of 323 older adults aged ≥65 years from rural areas of Korea participated. LUTS prevalence was evaluated and HRQoL was measured using the King’s Health Questionnaire. The chi-square test and t -test were used to examine sex differences in characteristics, LUTS, and HRQoL. Multivariable logistic regression was used to identify risk factors associated with UI.
Results
Nocturia was the most prevalent symptom, affecting 87% of men and 86% of women. Women (53%) had significantly more UI of any kind than did men (35%) (P=0.007). Urgency UI was the most frequent type of UI in men, whereas stress UI was the most frequent in women. Regarding HRQoL, men had significantly higher scores in the domains of sleep/energy disturbances (P=0.032) than did women, and women reported greater effects from the severity of incontinence (P=0.001) than did men. Arthritis was the only factor associated with UI in men (odds ratio [OR], 6.88; 95% confidence interval [CI], 1.46–32.36). However, women with diabetes mellitus were less likely to have UI than those without (OR, 0.43; 95% CI, 0.23–0.82).
Conclusions
LUTS were found to be highly prevalent in community-dwelling older Korean adults in rural areas. Interventions to improve sleep and to reduce UI severity are needed for incontinent men and women, respectively.
INTRODUCTION
According to the Korean Statistical Information Service, the life expectancy of Koreans at birth in 2014 was 82.4 years, and adults aged ≥65 years will account for 20% of the population by 2025 [1]. Additionally, the proportion of older adults is greater in rural areas than in Korea as a whole. As the older population increases, health care providers’ interest in lower urinary tract symptoms (LUTS) is also growing because LUTS increase with age [2,3]. LUTS can be categorised into storage, voiding, and postmicturition symptoms [4]. Storage symptoms include frequency, nocturia, urgency, and urinary incontinence (UI), and voiding symptoms include slow stream, splitting, intermittent stream, hesitancy, straining, and terminal dribble. A feeling of incomplete emptying and postmicturition dribble are postmicturition symptoms. According to population-based studies [2,3], older men have more voiding and postmicturition symptoms than do older women. Moreover, men aged ≥70 years have shown a higher prevalence of storage symptoms than women aged ≥70 years [3].
Among LUTS, UI is associated with nursing home admission, functional decline, and risk of death among community-dwelling older adults [5]. UI also negatively affects individuals’ health-related quality of life (HRQoL) [6]. Specifically, urgency UI decreases HRQOL more than other types of UI in older adults [6]. To date, however, little information is available on sex differences in LUTS, factors associated with UI, and HRQoL in older Korean adults exclusively living in rural areas.
The purposes of this study were to examine sex-related differences in the prevalence of LUTS and factors associated with UI in community-dwelling older adults living in rural areas and to explore HRQoL in incontinent older adults.
MATERIALS AND METHODS
Study Design and Sample
A cross-sectional design was used for this study of adults aged ≥65 years in rural areas of Korea. For data collection, face-to-face interviews were conducted at 15 rural community-health centres by research assistants who were nurses and received standardised training for data collection. The exclusion criteria were (1) the self-reported presence of symptoms of urinary tract infection, (2) receiving any treatment for LUTS, or (3) decreased cognitive function as assessed using the Korean version of the Mini-Mental State Examination-Dementia Screening [7]. A total of 380 adults participated, of whom 323 (men, 75; women, 248) met the inclusion criteria for this study. This study was approved by the Institutional Review Board of Yonsei University (2016-0004-1).
Measures
To collect information on LUTS, interviews were conducted using the questionnaire that was utilized in the study of Lee et al. [3], which was originally developed by Irwin et al. [2]. Participants were asked about storage symptoms (nocturia, frequency, urgency, UI), voiding symptoms (terminal dribble, slow stream, straining, intermittency), and postmicturition symptoms (incomplete emptying, postmicturition dribble).
Participants were considered to have UI if they answered “several times a week” or “every day” to the question “How often do you leak urine?” Participants with UI were then asked whether they had stress UI (“Do you experience urine leakage when you sneeze, cough, or exercise?”) and/or urgency UI (“Do you experience urine leakage when you have a sudden urge to urinate?”). Participants with both stress and urgency UI were considered as having mixed UI. Participants were considered to have overactive bladder (OAB) if they answered “yes” to the question “Do you experience sudden urges to urinate and have difficulty in holding urine?” and answered “several times a week” or “every day” to the question “How often do you have this experience?”
To measure HRQoL among participants with UI or OAB, defined as a feeling of urinary urgency with or without urgency UI, the Korean version of the King’s Health Questionnaire was administered [8]. This questionnaire was originally developed by Keller and colleagues in 1997 and consists of 21 items and 8 domains (general health perception, impact on life, role limitations, physical limitations, social limitations, personal relationships, emotions, sleep/energy), with a separate scale for measuring the severity of urinary symptoms [9]. Each item is scored on a 4-point scale, and the range of each domain is from 0 to 100, with a higher score indicating a greater impairment of HRQoL. The Cronbach alpha of this questionnaire in the current study was 0.858.
Information on the participants’ age; education; marital status; self-reported health status; self-reported comorbidities such as hypertension, stroke, arthritis, diabetes mellitus (DM), and benign prostatic hyperplasia (BPH); falls; and instrumental activities of daily living were collected. The participants’ height and weight were measured by a research assistant.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA). Descriptive statistics were used to describe the participants’ characteristics, LUTS, and HRQoL. We used the chi-square test and the t-test to examine differences in characteristics, LUTS, and HRQoL between men and women. Multivariable logistic regression was used to identify risk factors associated with UI.
RESULTS
The characteristics of the participants are described in Table 1. The average age of the participants was 77.4 years (standard deviation, 5.9), and 38% were ≥80 years old. Approximately 57% had no education, and 17% of the men and 69% of the women were illiterate (P<0.001). Three-quarters of the men and 41% of the women reported having a spouse (P<0.001). Hypertension was the most prevalent problem in both men (72%) and women (65%). Arthritis was the second most prevalent health problem and was significantly more prevalent in women than in men (P=0.045).

Comparison of characteristics and lower urinary tract symptoms between men and women
Nocturia, defined as waking at night ≥1 time to void, was the most prevalent LUTS and affected 87% of men and 86% of women (Table 1). When nocturia was defined as voiding ≥2 times per night, the prevalence was 61%. Women (53%) were significantly more often affected by UI of any type than men (35%) (P=0.007). Urgency UI was the most frequent type of UI in men, and stress UI was the most frequent in women. Regarding voiding symptoms, men reported significantly more terminal dribble (P<0.001), slow stream (P<0.001) and straining (P<0.001) than did women. Half of all participants experienced slow stream, which was the most prevalent voiding symptom in both sexes. Approximately 22% and 8% of the participants reported postmicturition symptoms of incomplete emptying and postmicturition dribble, respectively. Incomplete emptying (P=0.001) and postmicturition dribble (P=0.001) were both significantly more prevalent in men than in women.
The participants who had UI or OAB (men, 27; women, 133) responded to the King’s Health Questionnaire. All domain scores are presented in Table 2. Men had significantly higher scores for the domains of sleep/energy disturbances (P=0.032) than did women, and women reported greater effects from the severity of incontinence (P=0.001) than did men. The results of our multivariate logistic regression for risk factors associated with UI are shown in Table 3. Among the men, arthritis was the only factor associated with UI; having arthritis significantly increased the odds of UI among older men (odds ratio [OR], 6.88; 95% confidence interval [CI], 1.46–32.36). In contrast, women with DM were less likely to have UI than were women without DM (OR, 0.43; 95% CI, 0.23–0.82).
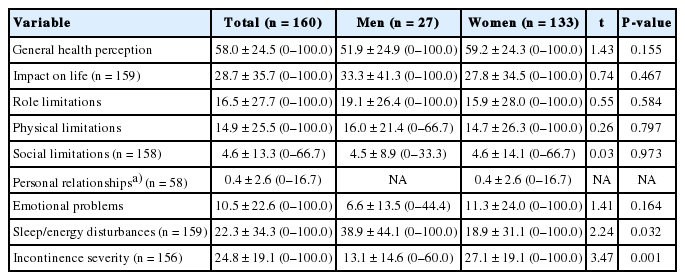
Comparison of health-related quality of life between men and women
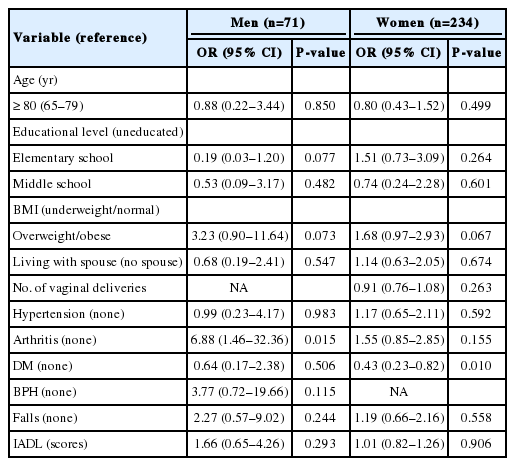
Factors associated with urinary incontinence in men and women
DISCUSSION
In this study, we confirmed that LUTS were highly prevalent in older Korean adults living in rural areas. In the literature, nocturia has been reported to be the most prevalent symptom in older adults, with a prevalence of approximately 71% when defined as voiding ≥1 time per night [2]. In contrast, the prevalence of nocturia has been reported to range from 36% to 52% when defined as voiding ≥2 times per night in adults aged ≥60 years [2,10]. Similarly, we found that the prevalence of nocturia was 86% and 61% using the former and latter definitions, respectively, and nocturia was the most-reported symptom.
UI has been reported to be more prevalent in older women (42%–52%) than in older men aged ≥65 years [11,12], which is consistent with our findings (34.7% in men and 53.2% in women). Among community-dwelling older adults, we found that arthritis significantly increased the odds of UI in men, but not women, unlike the results of previous studies [13]. We found that urgency UI was the most prevalent type of UI in men, which is consistent with the results of a previous study [14]. In the present study, arthritis was found to be significantly associated with UI in older men. A possible explanation for this finding is that men who have arthritis might take more time to reach the toilet than men without arthritis, possibly experiencing urine leakage on the way. Another interesting finding in the current study was that DM decreased the odds of UI in women. Similarly, Jackson et al. [15] found that women with diabetes reported less stress and urgency UI than women without diabetes. They also found that women with diabetes had less slight or moderate UI measured by the Sandvik severity index, and more severe UI than nondiabetic women. Therefore, a possible explanation for our finding is that women with diabetes and severe UI might have been excluded from the current study due to having experience of treatment, such as medication and/or surgery for UI, which was one of the exclusion criteria for our study. It is well established in the literature that the severity of UI in women is significantly associated with seeking treatment [16]. Since the severity of UI was not examined in our study, more studies investigating the association between DM and UI in older women are needed. Although significant associations of advanced age [17], being overweight/obese [18], falls [19], and BPH [20] with UI have been reported in the literature, we did not find any such associations.
The participants with UI or OAB in the current study reported better HRQoL in most domains of the King’s Health Questionnaire than in the study of Okamura et al. [21]. One possible explanation is that the participants in the study of Okamura et al. [21] were recruited at urology clinics; thus, their LUTS might have been more severe than those of our participants. Interestingly, however, the men in our study reported greater effects in the domain of sleep/energy disturbances than did those in the previous study. This finding might be associated with a higher prevalence of nocturia among the men in our study than was found among the men in the study of Okamura et al. Another interesting finding regarding the domain of sleep/energy disturbances was that the men had significantly lower HRQoL than the women, even though the prevalence of nocturia did not differ significantly between them. A study found an association between increased nocturnal voiding and subjective and objective sleep parameters [22], but that study also addressed obesity, sleep apnoea, fluid intake, and caffeine use, all of which could be associated with nocturnal voiding [23]. One possible explanation for our result is that older men might feel more exhausted or disturbed from waking to void at night than older women. Men had significantly more voiding and post-micturition symptoms such as slow stream, straining, and incomplete emptying than women; therefore, they might spend more time and effort to void than women.
Regarding sex differences in voiding symptoms, it has been found that voiding symptoms are more prevalent in men than in women. Cameron et al. [24] found that men had significantly more symptoms of weak stream (61% vs. 29%), intermittency (53% vs. 25%), hesitancy (48% vs. 24%), and straining (28% vs. 19%) than women. The Korean EPIC study also found that voiding symptoms were more prevalent in men aged 65 years or older, and the age group of 70–96 years had the largest difference in the prevalence of voiding symptoms between men and women [3]. In a similar vein, the current study found that 30% to 77% of men reported voiding symptoms, and most symptoms (except intermittency) were significantly more prevalent in men than in women.
This study had several limitations. First, we used the convenience sampling method, defined as a selection of the most readily available persons as participants in a study [25], to recruit older adults. Thus, older adults with LUTS might have been overrepresented in our sample.
Second, reporting bias could have been present. Data collection was conducted by a research assistant through face-to-face interviews; thus, the participants’ reported LUTS might have differed from their real symptoms. Face-to-face interviews for data collection seemed to be appropriate because approximately half of the participants were illiterate; however, it is possible that some of participants might not have accurately reported their LUTS because they might have considered LUTS to be an embarrassing condition [26]. Third, the information on the participants’ health problems was self-reported and was not medically assessed, which might have led to inaccuracies in the data; therefore, our results must be carefully interpreted. For example, some of the men might have had undiagnosed early symptoms of BPH. Thus, the use of self-reported health conditions might have resulted in a weakened association between BPH and UI in men.
Finally, the current study included fewer men than women, which might have biased the results. Although the proportion of women to men aged 70–99 in the rural areas where we conducted the study was about 100 to 82 in 2016 [1], the sex ratio of women to men in the current study was about 3 to 1. Therefore, careful interpretation of the results and more studies of sex differences in LUTS, using more representative sex ratios, are needed.
Despite these limitations, this study provides valuable information. This study focused on older adults living in rural areas; therefore, it provides useful information on the possible effects of characteristics of rural areas on LUTS. The rural area where we conducted this study is a province where the proportion of older adults is much greater than the average proportion in Korea as a whole (22% vs. 13%, respectively). As older adults living in rural areas have relatively limited access to health care specialists and because their characteristics, such as educational level and living environment, are different from those of older adults living in cities or metropolitan areas (e.g., living in a single house vs. an apartment), information about their self-reported LUTS can provide baseline data for designing and providing person-centred interventions. The current study highlights that nocturia was the most prevalent LUTS in both sexes in rural areas. Thus, applying interventions to reduce nocturia would be important. Both behavioural interventions, such as restricting fluid intake and caffeinated drinks in the evening, and environmental interventions, such as providing a bedside commode, could be considered. Regarding arthritis, which was a factor associated with UI in men, health care providers should pay attention to UI in older men with arthritis.
In conclusion, LUTS were highly prevalent in older Korean adults living in rural areas. Interventions to improve sleep and to reduce UI severity are needed in men and women, respectively.
Acknowledgements
The authors would like to thank 15 community health nurse practitioners in Gapyeong-gun for their valuable help.
Notes
Grant/Fund Support
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (No. 2015R1C1A1A01054434).
Research Ethics
This study was approved by the Institutional Review Board of Yonsei University (2016-0004-1), and written informed consent was obtained from all participants.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
· Full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis: JP
· Study concept and design: JP, YJL, HSL, JTS
· Acquisition of data: JP, ESK
· Analysis and interpretation of data: JP, ESK
· Drafting of the manuscript: JP, YJL
· Critical revision of the manuscript for important intellectual content: JP, YJL, HSL, JTS
· Statistical analysis: JP, ESK
· Obtained funding: JP
· Administrative, technical, or material support: JP, ESK
· Study supervision: JP