Bicycle Riding: Impact on Lower Urinary Tract Symptoms and Erectile Function in Healthy Men
Article information
Abstract
Purpose
Recently, reports in the mass media have implicated that bicycle riding increases the risk of erectile dysfunction and prostatic diseases. So, we evaluate the impact of bicycle riding on erectile function and lower urinary tract symptoms (LUTS) in healthy general men.
Methods
From 26 June 2010 to 20 July 2010, we investigate degree of LUTS (voiding and storage symptoms), using International Continence Society-male Questionnaire (ICS-mQ) and erectile function using International Index of Erectile Function-5 Questionnaire (IIEF-5) in 5 work places (personnel of public office, hospital, university, etc.) of which bicycle riding club members were doing active club activities. Respondents, who participated in club activities for 6 months and longer, were classified as the bicycle club (142 men; age, 44.02±8.56). Ones who do not ride bicycles were classified as the control group (83 men; age, 42.13±7.85). People who were having the history of urological and other chronic diseases (diabetes, vascular disease, heart disease, etc) were excluded from both groups.
Results
Bicycle club is not significantly associated with increased prevalence of LUTS (bicycle club, 2.1 to 57.7% control, 4.8 to 73.5%) and erectile dysfunction (bicycle club, 46.1% control, 55.4%). The total mean score (storage/voiding/erectile function) of bicycle club (13.93±1.95/11.14±3.49/20.46±5.30) were not significantly different from control (14.35±2.49/11.52±3.38/20.40±4.07) (P=0.190 to 0.968).
Conclusions
These results suggested that bicycle riding as exercise or hobby has no negative effect on LUTS and erectile function in healthy general men, although this research data were limited to the questionnaire analysis.
INTRODUCTION
Bicycle riding is twice more effective than walking for exercising. In particularly, it was reported that because walking or jogging strains knee joints, bicycle riding is more suitable for people who areobese, infirm, osteoporoticor have joints problem. Like any other aerobic exercises, bicycle riding is readily available and is economical and efficient form of aerobic non-impact exercise with established cardiovascular beneficial effects [1,2].
As a forementioned, there is no doubt that bicycle riding is good exercise. Nevertheless, it has been reported that bicycle riding negatively affects the urogenital system or erectile function. Therefore, some people hesitate to start bicycle riding as exercise [3,4]. In most cases, however, such studies have been conducted on professional cyclists who put excessive pressure on their perineal regions while they are riding bicycles or horsebacks. Thus, it is hard to apply the results to amateurs who do bicycle riding as a hobby or recreation.
Hereat, we conducted a survey of voiding and storage symptoms and erectile function on bicycle riding club members and non-members in order to investigate whether bicycle riding actually has negative effect on LUTS and erectile function.
MATERIALS AND METHODS
A self-administered survey was conducted from June 26 until July 20, 2010 at five workplaces (one public office personnel, two university hospitals and two universities). All subjects were selected randomly and agreed to answer the questionnaire. Two groups were designed. One group of people was bicycle riding club members (bicycling club), and the other group was people who had not riddenbicycles for a long time (control). Bicycling club was limited to people who were participating club activities for the last six months and longer. The survey was carried out by an experienced agent. To compare demographic characteristics, individual body mass index, marital status, years of bicycle riding, bicycle riding hours per day, sedentary live hours per day and comorbidities were investigated. People with neurologic abnormalities, history of chronic diseases such as diabetes, hypertension and heart diseases or those who have been treated for urologic diseases related with bladder, prostate or urethra within recent one year were excluded from this study. The bicycle riding hours were classified into three parts: daily hours, weekly frequency and weekly hours (daily hours×weekly frequency). The daily hours was rated a scale of 0.5 to 3; 0.5 (less than 30 minutes), 1 (less than 60 minutes), 2 (less than 120 minutes) and 3 (120 minutes and longer). The weekly frequency was rated from 1 to 6; 1 (less than 1 time), 2 (1 to 2 times), 4 (3 to 4 times) and 6 (5 times and over).
The International Continence Society Male Questionnaire (ICS-mQ) and the International Index of Erectile Function-5 (IIEF-5) were used to evaluate LUTS (voiding and storage symptoms) and erectile function respectively [5,6]. ICS-mQ consisted of 34 items in all; 22 relevant to lower urinary tract symptoms, 4 to sexual function, 7 to the quality of life and 1 subjective question. Among the 22 items relevant to LUTS, 8 questions were about urinary voiding; 10 about urinary storage; 3 about the pattern of urination; and 1 about post-voiding dribbling. Each objective question had four to five examples. In this study, the survey was carried out with the 18 questions about urinary voiding and storage symptoms. IIEF-5 consisted of five items to inquire into erectile confidence, full erection, erectile maintenance, erectile durability and sexual satisfaction during the last six months. Each symptom was rated from one to five points. An inter-group comparison was made in relation to the five items. Positive symptoms of LUTS and erectile dysfunction were as follows: frequency (time/day), 8<; frequency (hr), <3; nocturia (time), 1≤; all other 15 symptoms of LUTS, sometimes ≤; erectile dysfunction, <22 points of total IIEF-5.
The program 'SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA)' was used for statistical analysis. The independent t-test was used to make a comparison of urinary voiding, storage and erectile function. In addition, Pearson chi-square test or Fisher's exact test was used to analyze the correlation with prevalence of LUTS and erectile dysfunction (ED) between bicycling club and control. The statistical significance level was defined as where the P-value was being less than 0.05.
RESULTS
Demographic Characteristics
The respondents were 225 men in all, 142 and 83 of whom were bicycling club and control group respectively. The average age of bicycling club members was 44.02±8.56 (25 to 62 years), and control-group was 42.13±7.85 (25 to 61 years) (P=0.079). In bicycling club members, 60 (42.3%) spent less than 5 hours a week riding bicycles; 44 (31.0%) spent 6 to 10 hours; 22 (15.5%) spent 11 to 15 hours; 13 (9.2%) spent 16 to 20 hours; 3 (2.1%) spent 21 hours and longer. There was no significant inter-group difference in demographic characteristics (Table 1).
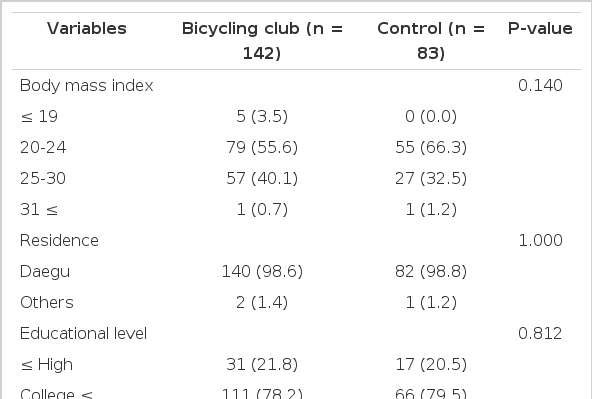
Sociodemographic characteristics of bicycling club and control
Prevalence of LUTS and ED
The prevalence of LUTS of each 18 voiding and storage symptoms on ICS-mQ were 2.1 to 57.7% in bicycling club and 4.8 to 73.5% control group (Table 2). The prevalence of ED (<22 points) on IIEF-5 were 46.1% in bicycling club and 55.4% in control group (P=0.071).
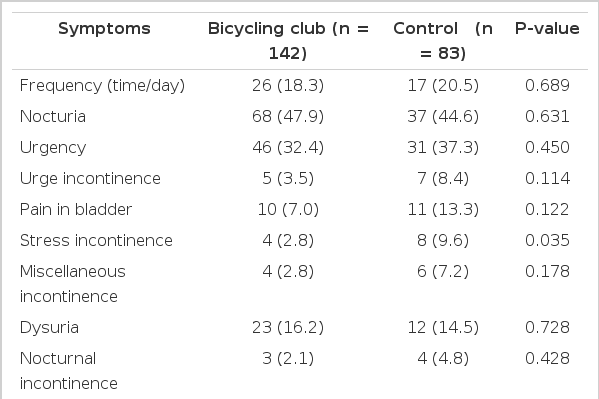
Prevalence of lower urinary tract symptom on ICS-mQ
Lower Urinary Tract Symptoms
In the questions of terminal dribbling (ICS-mQ no.18), the two groups showed significant differences (P=0.035) (Table 3). However, in relation to total urinary storage, urinary voiding symptoms evaluated by ICS-mQ, bicycling club members scored 13.93±1.95 and 11.14±3.49 points respectively. Control-members scored 14.35±2.49 and 11.52±3.38 respectively. There was no significant inter-group difference (P=0.190 to 0.408) (Table 4).
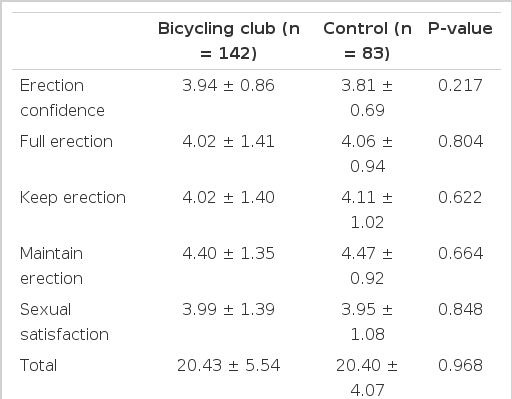
Erectile function in bicycling club and control group

Lower urinary tract symptom in bicycling club and control group
Erectile Function
In relation to erectile function evaluated by IIEF-5, the two groups showed no significant differences in erectile confidence, full erection, keep erection, maintain erection and sexual satisfaction (P=0.217 to 0.848) (Table 3).
DISCUSSION
The reported urogenital symptoms that is related with bicycle riding varies considerably. The most common urogenital symptoms are genitalia numbness, followed by erectile dysfunction. Other less common symptoms which include priapism, penile thrombosis, infertility, hematuria, torsion of spermatic cord, prostatitis, perineal nodular induration and elevated serum prostate-specific antigen (PSA) are reported only sporadically. However, the above studies were conducted on professional cyclists or people who had ridden mountain bikes for a long distance [7].
In previous studies of lower urogenital symptoms, it has been reported that strenuous and long-distance bicycle riding might cause prostatitis, the perineal pains and the increase in serum PSA because of direct pressure on the perineum and prostate [7-9]. Mechanical stress of the prostate caused by movement of the pelvic muscles or direct perineal pressure produced by the saddle with a significant massage influence on the prostate [8]. On the other hand, Crawford et al. [10] reported that statistically or clinically significant increase in serum PSA level were not observed following a 4 day 250-mile bicycle riding. Even though the influence of bicycle riding on the lower urinary tract is still controversial, only a few studies has been established based on authorized scales, at least in PubMed.
Horseback riding is cited as an exercise that puts pressure on the perineal region like bicycle riding. In a study, a comparison was made between horseback riding club members and swimming club members in LUTS. In result, the two groups did not show significant differences in American Urological Symptom Index of Urinary Symptom and IIEF-5 [11]. The result implies that people who enjoy horseback riding as a hobby do not need to be afraid of having problem with their lower urinary tracts or getting ED [11]. Likewise, bicycling club and control-members did not show significant differences in prevalence and symptoms of LUTS in the study. It implies that bicycle riding does not exert negative influence on the lower urinary tract to amateur bicycle riders, unlike professional cyclists or people who ride bicycles strenuously.
Weiss [3] has reported that transient perineal numbness was occurred to 45% of people during an 8-day 804.97-km bicycle tour and 2% of them had to temporarily stop riding bicycle. Andersen and Bovim [4] has conducted a cross-sectional study on 160 professional cyclists who participated in a 540-km race and reported that ED was occurred to 21 participants (13%). Perineal numbness may occur without having ED although ED from cycling is invariably associated with perineal numbness, which may serve as a marker for increasing the risk of suffering from ED [7]. Even though the cause of ED from bicycle riding is not fully understood, a result of continuous compression and strain on the pudendal nerve and arteries that leads nerve entrapment and vascular occlusion is one of theories [12].
In the study, an analysis was made of how bicycle riding would affect erectile function to common people who ride bicycles as a hobby. Marceau et al. investigated the correlation between the bicycle riding and ED with 1,709 subjects (40 to 70 years) that were composed of long-distance bicycle racer and people who rode bicycles as a recreation or a means of transport. In results of the study, bicycling less than three hours per week was not associated with ED but somewhat protective. However, bicycling three hours or more per week may associate with ED [13]. Alanee et al. [11] compared horse riding club and swimming club members by using IIEF-5, but they did not differ from each other in erectile function. Likewise, our study showed that total and each five item score of IIEF-5 were not significantly different in bicycling club, compared to control group.
In the case of our study, the number of surveyees was not enough to generalize the results. An analysis was made whether the cycling frequency and cycling hours affects to LUTS and erectile function, but significant correlations were not observed. Most of bicycling club members (104) spent their time for the riding bicycle six to ten hours a week. Only 11.2% of the club members rode bicycle 16 hours and longer a week. Another limitation of our study is that the research data was made only from the questionnaire analysis. Therefore, further research of underlying factors that leads to prostate disease and ED by large-scale is needed.
In conclusion, the results of this study show that bicycle riding has no negative effect on LUTS and erectile function at least in healthy ordinary men who enjoy bicycle riding as a hobby. It requires that further studies should be conducted with more participants.
Notes
No potential conflict of interest relevant to this article was reported.