Increased Bladder Wall Thickness in Diabetic and Nondiabetic Women With Overactive Bladder
Article information
Abstract
Purpose:
Bladder wall thickness has been reported to be associated with overactive bladder (OAB) in women. Diabetic women have an increased risk for OAB syndrome and may have an increased risk for bladder wall thickness.
Methods:
A total of 235 female patients aged 40 to 75 years were categorized into four groups. The first group consisted of women free of urgency or urge urinary incontinence. The second group included nondiabetic women with idiopathic OAB. The third group consisted of women with diabetes and clinical OAB, and women with diabetes but without OAB constituted the fourth group. Bladder wall thickness at the anterior wall was measured by ultrasound by the suprapubic approach with bladder filling over 250 mL.
Results:
The diabetic (third group) and nondiabetic (second group) women with OAB had significantly greater bladder wall thickness at the anterior bladder wall than did the controls. However, the difference was not significant between the diabetic (third group) and the nondiabetic (second group) women with OAB. Women with diabetes but without OAB (fourth group) had greater bladder wall thickness than did the controls but this difference was not significant. Additionally, the difference in bladder wall thickness between diabetic women with (third group) and without (fourth group) OAB was not significant.
Conclusions:
This is the first study to show that bladder wall thickness is increased in diabetic women with and without OAB. Additionally, nondiabetic women with OAB had increased bladder wall thickness. Further studies may provide additional information for diabetic and nondiabetic women with OAB, in whom the etiopathogenesis of the disease may be similar.
INTRODUCTION
Evidence suggests an increased prevalence of urgency with or without urge urinary incontinence among women with type 2 diabetes [1] and an increasing trend with longer duration of diabetes [2]. Overactive bladder (OAB), a highly prevalent and disturbing disease, is also based on the symptoms of urgency, with or without urge urinary incontinence, usually with frequency and nocturia [3]. Although urodynamic studies are widely used in patients with symptoms of OAB, only 54% show detrusor overactivity on conventional urodynamics [4]. Similarly, 55% of diabetic patients with OAB and 25% of asymptomatic patients with diabetes show detrusor overactivity during urodynamic studies [5,6].
Bladder wall thickness has been shown to be significantly increased in women with detrusor overactivity [7]. This variable has also been applied in the assessment of voiding dysfunction, bladder outlet obstruction, and as a screening tool in the assessment of upper urinary tract deterioration in children with myelodysplasia [8,9]. In animal studies, diabetes has been shown to result in hypertrophy of the bladder wall with an increase in smooth muscle and urothelium thickness [10]. Diabetic women with OAB may also have an increased risk for bladder wall thickness, which may have prognostic potential.
We aimed to investigate the association of bladder wall thickness in diabetic and nondiabetic women with OAB and to discuss the possible common underlying mechanisms.
MATERIALS AND METHODS
Study Population
This study was cross-sectional and was conducted in our urology department. Women aged 40 to 75 years old with or without lower urinary tract symptoms were categorized into four groups. The first group consisted of nondiabetic women free of urgency or urge urinary incontinence without complaints related to urological diseases. The second group included nondiabetic women with clinical OAB. Participitants in this second group consisted of nonneurogenic patients with no history of diabetes and normal glucose levels with idiopathic OAB syndrome. Women with known diabetes mellitus who were referred to our clinic from the endocrinology department were classified into the final two groups: women with diabetes and clinical OAB syndrome made up the third group, and women with diabetes but without OAB constituted the fourth group.
Female patients with urinary tract infection, concurrent neurologic disorders such as Parkinson disease, multiple sclerosis, spinal cord injury, or stroke were excluded. Women were also not enrolled if they were taking medication that could affect bladder function, such as diuretics or calcium channel blockers. Patients who currently or who had previously used antimuscarinics were also excluded to avoid a likely effect on bladder wall thickness. Women with evidence of significant pelvic organ pro-lapse quantified by a pelvic organ prolapse quantification system (POP-Q) score of greater than 1 in the anterior, posterior, or cervical/vault components of the scoring system; bladder outlet obstruction; or with residual volume over 20 mL were not included at the time of enrollment. We also needed to exclude a few patients in whom suprapubic measurement of the bladder wall was not practicable by ultrasound because of morbid obesity.
Demographic characteristics such as age, medical history, and comorbidities were obtained. A pelvic examination was performed in women with symptoms of OAB. Body weight, height, and visceral obesity were recorded and the BP of patients who were not on current drug therapy was measured during the clinical examination. All female patients with OAB symptoms (second and third groups) had urge urinary incontinence.
The women who agreed to participate in the study completed a 3-day frequency-volume chart and quality of life measures including the OAB Validated 8-question screening tool (OABV8). Patients with scores of 8 or higher were acknowledged to have OAB. OAB syndrome was defined according to the International Continence Society 2010 definition as urinary urgency, usually accompanied by frequency and nocturia, with or without urge urinary incontinence, in the absence of urinary tract infection or other obvious pathology [3]. Metabolic syndrome was defined according to the 2006 International Diabetes Federation criteria as waist circumference of 80 cm in female patients and two or more of the following: fasting plasma glucose, ≥100 mg/dL, serum triglyceride level, ≥150 mg/dL; serum high-density lipoprotein cholesterol level, <50 mg/dL or specific treatments for any of these lipid abnormalities; and systolic blood pressure (BP), ≥130 mmHg and/or diastolic BP, ≥85 mmHg [11].
This study was approved by the local ethics committee and informed consent was obtained from all patients before participation in the study.
Ultrasound Examination
All ultrasound measurements were performed by the same radiologist using the Toshiba, Xario (Toshiba, Tokyo, Japan) with the abdominal 7.5 Mhz probe PVT375BT and with the patient in a supine position. The radiologist was blinded to the patient’s lower urinary tract symptoms during the ultrasound examination. The measurement was performed by applying the ultra-sound probe suprapubically without pressure. All measurements were enlarged five-fold with the bladder wall being measured perpendicular to the luminal surface of the bladder in the anterior bladder wall (Fig. 1).

Measurement of bladder wall thickness at the anterior wall with bladder filling over 250 mL.
The Oelke technique [8] was used for the measurement of bladder wall thickness. The patients were asked to wait until they felt a desire to void. Bladder wall thickness at the anterior wall was measured with bladder filling over 250 mL and was recorded (Fig. 1). Then, the patients were asked to void. Participants with residual volume over 20 mL or with a bladder capacity less than 250 mL during the ultrasound examination were not enrolled.
Biochemical Analysis
Blood samples were drawn from all subjects after they had fasted overnight. Serum concentrations of glucose, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglycerides were measured by automated enzymatic photometry (Architect ci16200, Abbott Laboratories, Abbott Park, IL, USA).
Statistical Analysis
Continuous variables were summarized as mean±standard deviations (SDs). Data were tested for normal distributions by using the Kolmogorov-Smirnov test. One way analysis of variance was used for the univariate analysis of the continuous variables. Statistically significant relationships were ascertained by using the Tamhane’s post hoc test. All tests of significance were two-tailed. Regression analysis was used to evaluate the association of clinical parameters and bladder wall thickness. Statistical significance was defined as P<0.05. PASW ver. 18.0 (IBM Co., Armonk, NY, USA) was used for all statistical calculations. Power calculations were not done because no preexisting data were available for these subjects.
RESULTS
We recruited 235 women to the study, all of whom underwent measurement of bladder wall thickness. The first group consisted of 46 nondiabetic women without OAB (controls; mean age, 55.8 years), and the second group included 65 nondiabetic women with OAB syndrome (mean age, 53.2 years). The third and fourth groups included 61 (mean age, 58.6 years) and 63 (mean age, 56.5 years) diabetic women with or without OAB syndrome, respectively. The demographic characteristics of the patients are shown in Table 1. The incidence of metabolic syndrome differed significantly among the groups: 35.9% of the controls met the criteria for metabolic syndrome compared with 64.7% of non-diabetic women with OAB, 92.4% of diabetic women with OAB, and 76.6% of diabetic women without OAB, respectively. In the regression analysis, none of these clinical factors was found to be associated with bladder wall thickness (Table 2).
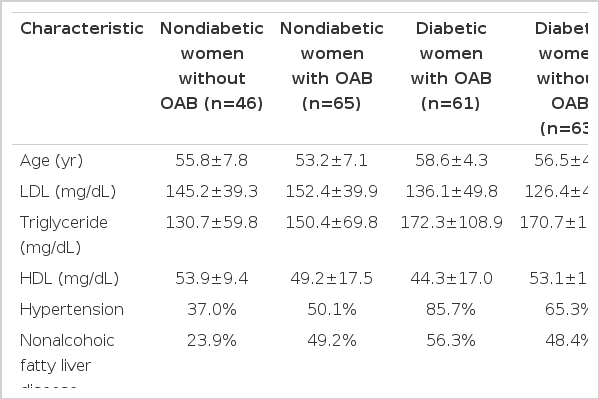
Demographic characteristics of the patients in the four study groups

Regression analysis of clinical parameters with bladder wall thickness
The statistical significance of the bladder wall measurements is shown in Table 3. Both the diabetic (third group) and the nondiabetic (second group) women with OAB had significantly higher bladder wall thickness at the anterior bladder wall than did the controls. However, the difference was not significant between the diabetic (third group) and nondiabetic (second group) women with OAB. The fourth group, which consisted of diabetic women without OAB, had greater bladder wall thickness than did the controls, but this difference was not significant. In addition, the diabetic women without OAB did not demonstrate significantly higher bladder wall thickness than that of the diabetic women with OAB (third group). Moreover, the nondiabetic women with OAB (second group) did not have greater bladder wall thickness than the diabetic women without OAB (fourth group).

Bladder wall thickness and statistical relations across diagnostic categories
DISCUSSION
Our results revealed a significant association between nondiabetic (idiopathic) OAB and bladder wall thickness. In addition, we found that diabetic women with OAB syndrome had significantly increased bladder wall thickness compared with controls. However, no significant difference was found between the diabetic and nondiabetic women with OAB. Moreover, no significant difference was found between the diabetic women without OAB syndrome and the nondiabetic women without OAB. We suggest that OAB syndrome causes bladder wall thickening regardless of whether the woman is diabetic; however, diabetes alone without OAB syndrome does not significantly increase bladder wall thickness.
We measured bladder wall thickness according to the Oelke technique [8]. Oelke [8] showed that in healthy women, detrusor wall thickness decreases rapidly between 50 and 250 mL of bladder filling but reaches a plateau thereafter with insignificant differences between 250 mL and maximum bladder capacity. This technique has the advantage that catheterization is not necessary. Suprapubic measurement of bladder wall thickness is widely preferred by most urologists. However, most gynecologists use a transvaginal route with bladder filling of less than 50 mL. Panayi et al. [12] used a transvaginal approach and found a relation with bladder wall thickness and OAB and also with the components of OAB syndrome. However, suprapubic measurement in empty bladders may reveal ambiguous results. The measurement approach and bladder filling during ultrasound examination shows great discrepancies among studies; therefore, we need further trials for standardization of the measurement technique.
It is assumed that repetitive involuntary contractions of the detrusor muscle during the storage phase while the urethral sphincter is closed result in hypertrophy of the detrusor and manifest as bladder wall hypertrophy [13]. On the other hand, metabolic syndrome (a cluster of visceral obesity, hypertension, glucose intolerance, and dyslipidemia) has been associated with OAB in females [14]. Metabolic syndrome is a prediabetic state that is associated with oxidative stress, inflammation, and chronic ischemia and that has been advocated in the etiopathogenesis of OAB [15,16]. In fructose-fed rats, a common model used for the study of metabolic syndrome, detrusor overactivity has been shown and histological examination revealed leukocyte infiltration around the endothelium of vessels and into the interstitial tissue, hypoxia, and fibrosis [17]. In addition to chronic inflammation-related fibrosis, animals with chronically ischemic bladder showed enhanced detrusor overactivity and increased collagen deposition [18]. We suggest that both chronic inflammation and ischemia may result in bladder wall thickness. Furthermore, metabolic syndrome-related insulin resistance and oxidative stress reduce nitric oxide production [19]. Nitric oxide has been shown to inhibit bladder smooth muscle cell growth [20]. Long-term nitric oxide deficiency has been reported that reduces beta-adrenoreceptor-mediated detrusor smooth muscle relaxations and results in detrusor overactivity [20] and that may also cause smooth muscle cell proliferation. Additionally, metabolic syndrome-related insulin resistance is associated with an increase in the level of insulin-like growth factor 1 (IGF-1). IGF-1 mRNA has been found to be increased in the urinary bladder during hypertrophy of smooth muscle and has been suggested to play a role in the hypertrophy of bladder smooth muscle cells [21]. Moreover, it has been shown that as a prediabetic state, rabbits with metabolic syndrome developed fibrosis [22] and that diabetes caused hypertrophy of the bladder wall and an increase in smooth muscle and urothelium thickness [10]. We suggest that urothelium thickness is a substantial component of bladder wall thickness, and hence, bladder wall measurement can be a better indicator than detrusor wall measurement. In summary, metabolic syndrome and related insulin resistance, chronic inflammation, oxidative stress, and chronic ischemia may cause an increase in collagen content, inflammation, fibrosis, and smooth muscle cell proliferation and hypertrophy. These pathogenetic interactions may result in bladder wall thickening. Because diabetes is the progressive form of metabolic syndrome, these mechanisms are likely responsible for the increase in the thickness of the bladder wall in diabetic patients.
Several potential study limitations should be noted. OAB was diagnosed on a clinical basis and urodynamic studies were not performed. Additionally, we excluded patients with residual volume over 20 mL, and diabetes mellitus may cause detrusor underactivity with a longer duration of diabetes. Whether alterations in bladder wall thickness occur with duration of diabetes mellitus is not known and could have affected our results. Meanwhile, suprapubic measurement of bladder wall thickness is not very applicable in women with morbid obesity, which may hinder the feasibility of this method.
This is the first study to show that bladder wall thickness is increased in diabetic women with OAB. Additionally, nondiabetic women with OAB had increased bladder wall thickness. Further studies may provide additional information for diabetic and nondiabetic women with OAB, in whom the disease may have similar etiopathogenesis.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.