Benign Prostatic Hyperplasia and the Risk of Falls in Older Men: Insights From a Population-Based Study on Geriatric Morbid Conditions
Article information

Abstract
Purpose
The purpose of this study was to explore the association between benign prostatic hyperplasia (BPH) and the incidence of falls from the perspective of geriatric morbid conditions.
Methods
Data were sourced from the triennial National Survey of Older Koreans conducted by the Ministry of Health and Welfare (2017–2020). In total, 8,135 male participants aged 65 and older were included, and information was gathered through questionnaires and physical measurements. Logistic regression analysis was utilized to determine the impact of BPH on the risk of falls, and subgroup analyses were conducted to examine the influence of BPH on specific types of falls.
Results
Of the participants, 15.2% (1,238 of 8,135) reported that their BPH treatment exceeded 3 months, and 8.0% (648 of 8,135) reported experiencing falls, with 61.4% (398/648) of these falls resulting in injuries. A significant association was identified between BPH and both falls (odds ratio [OR], 1.798; 95% confidence interval [CI], 1.479–2.185) and falls with injuries (OR, 2.133; 95% CI, 1.689–2.694). A subgroup analysis indicated a correlation between BPH and falls in groups having one (OR, 1.912; 95% CI, 1.356–2.694) and 2 or more conditions (OR, 1.856; 95% CI, 1.455–2.367) involving visual and auditory impairments, cognitive decline, depression, lower motor weakness, and limitations in daily activities.
Conclusions
The findings indicate that BPH contributes to the incidence of falls among older men, particularly those with comorbid conditions. Considering the heightened fall risk among elderly individuals suffering from multiple morbidities, particularly those with BPH, targeted interventions are essential for mitigating the risk of falls in this vulnerable group.
INTRODUCTION
Falls represent the primary cause of injuries in individuals aged 65 and older [1,2]. These injuries, influenced by chronological aging and gender, result in additional healthcare utilization, expenses, and a lasting decrease in overall quality of life [3]. Additionally, falls can lead to severe injuries, including damage to internal organs, lower extremity injuries, and traumatic brain injuries, sometimes resulting in fatal outcomes. Such fatalities are more common in older men and tend to increase with age [4]. Notably, emergency room visits due to falls among older persons exhibited an upward trend, reaching 68.8% in 2010 and showing annual increases thereafter [5]. More than 50% of injury-related hospitalizations among people over 65 years are due to falls. Fall-related injuries are also accompanied by shortand long-term functional impairment, leading to a consequent reduction in quality of life among older adults [6].
Benign prostatic hyperplasia (BPH) also has significant implications for male health and well-being. BPH becomes more prevalent with age and may exacerbate the reported severity of lower urinary tract symptoms (LUTS) in older individuals [7,8]. Numerous studies have indicated that BPH and related LUTS can significantly impact the incidence of falls [9-13]. Given the multiple factors impacting BPH and falls, it is crucial to investigate the relationship between falls and BPH across a wide range of representative demographic populations to ensure a comprehensive understanding. In the present study, our objective was to investigate this relationship utilizing data from the National Survey of Older Koreans. This survey is conducted through face-to-face interviews with experienced examiners and is designed to gather comprehensive information from individuals, specifically those aged over 65 years. Our study particularly emphasized the functional determinants of falls, encompassing factors such as impairments in hearing and vision, cognitive function, depression, lower muscle strength, and limitations in daily activities. These factors are hypothesized to contribute to the occurrence of falls and fall-related injuries.
MATERIALS AND METHODS
Study Participants
The National Survey of Older Koreans is a cross-sectional study conducted nationwide, encompassing older adults using population-based sampling in the Republic of Korea. This study has been carried out in 3-year cycles since 2008 under the auspices of the Ministry of Health and Welfare. Employing a stratified sampling approach based on residence district, the investigators conducted surveys targeted at older individuals aged 65 years and above. For this study, we focused on data for 2 survey cycles, conducted from 2017 to 2020. Among the 20,396 participants, we excluded female participants (n=12,233), participants who did not respond to the fall-related questionnaire (n=19), and those with missing anthropometric data (n=9). Consequently, we gathered information from 8,135 male participants for the purposes of our research.
Evaluation of BPH and Falls
BPH was defined as a positive response to the question: “Have you been diagnosed with BPH and treated by a physician for a duration exceeding 3 months?” Falls were defined as any instances of falling within a 1-year period preceding the survey. To assess the risk of falls, we utilized data from questionnaires that inquired about the “utilization of medical services due to fall-related injuries.”
Potential Confounders
The study posited that a higher number of morbid conditions for falls could potentially strengthen the link between BPH and the prevalence of falls. To explore this, the research focused on prevalent coexisting conditions often found in the geriatric population. These included issues related to visual and auditory impairments [14], cognitive decline [15], depression [16], diminished lower motor function [17], and restrictions in daily activities [18,19]. To test the hypothesis, the study categorized participants into groups based on their risk factors, segmenting them as having zero, one, or 2 or more risk factors.
In this study, we defined visual and auditory impairment as the experience of discomfort related to vision or hearing, as well as the use of assistive devices. Cognitive decline was defined as a score below the age-stratified threshold on the Korean version of the Mini-Mental State Examination for Dementia Screening (MMSE-DS) or a clinical diagnosis of Alzheimer disease. Depression was assessed using the Korean version of the Short Form Geriatric Depression Scale, with a diagnosis being established when a participant scored 8 or higher [20]. Lower motor weakness was evaluated based on the ability to perform 5 consecutive sit-to-stand movements on a chair, a measure commonly utilized in various research works to assess the risk of falls. To evaluate limitations in daily activities, we employed a set of criteria that included both activities of daily living (ADL)—tasks such as dressing, washing one’s face and hands, bathing, eating, transferring, toileting, and maintaining continence—and instrumental ADL, which encompass activities such as grooming, housework, meal preparation, laundry, taking short trips, using transportation, shopping, managing finances, and using the telephone. Individuals were classified as experiencing limitations in daily activities if they responded affirmatively to any of the questions, indicating a need for either “some assistance” or “a significant amount of assistance.”
Statistical Analysis
To assess the significance of differences, chi-square analysis was used for categorical variables, and the Student t-test was utilized for continuous variables. Logistic regression analysis was conducted to compare the impact of fall types on BPH while adjusting for the following variables: age, body mass index (BMI), living arrangement, years of education, number of chronic diseases, the number of medications used, visual and auditory impairments, lower motor weakness, and limitations in daily activities. For subgroup analyses, multivariate logistic regression analysis was performed to investigate the association between BPH and falls in individuals with various morbid conditions. To determine the relative prevalence of falls in relation to BPH and the 3 categories of morbid conditions, prevalence rates and standard errors were calculated. All statistical analyses were carried out using IBM SPSS Statistics ver. 27.0 (IBM Co., Armonk, NY, USA) and R ver. 4.0 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Baseline Characteristics
The study included a total of 8,135 participants. Among these, 8.0% (648 of 8,135) reported experiencing at least one fall within the past year, and 4.9% (398 of 8,135) reported falls resulting in injuries. Furthermore, 13.9% (1,238 of 8,135) of respondents were diagnosed with BPH. The cohort had the following characteristics: 41.8% (3,398 of 8,135) were aged 75 years or older, 54.3% (3,706 of 8,135) resided in urban areas, 13.2% (1,070 of 8,135) lived alone, 22.8% (1,852 of 8,135) had a BMI of 25 kg/m² or higher, 56.0% (4,553 of 8,135) had been diagnosed with hypertension, 16.7% (1,362 of 8,135) had been diagnosed with dyslipidemia, 23.2% (1,890 of 8,135) had been diagnosed with diabetes mellitus, 21.5% (1,748 of 8,135) were current smokers, and 30.0% (2,439 of 8,135) were current drinkers. Table 1 provides a detailed summary of the participants’ characteristics.
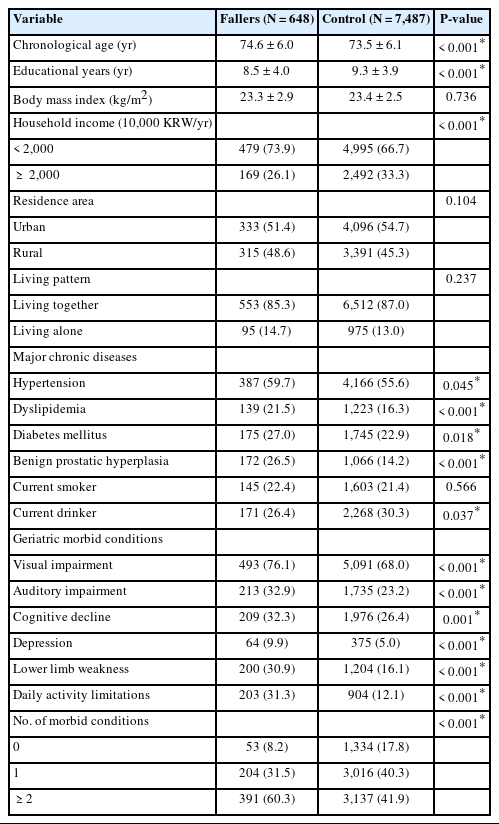
Participants’ characteristics from the National Survey of Older Koreans
Logistic Regression Analysis
In the logistic regression analysis, BPH was associated with a significantly higher prevalence of falls (odds ratio [OR], 2.177; 95% confidence interval [CI], 1.807–2.622; P<0.001) and falls with injuries (OR, 2.600; 95% CI, 2.079–3.252; P<0.001) when compared to participants who had not fallen. After adjustments, the ORs for any falls and falls resulting in injuries were 1.798 (95% CI, 1.479–2.185; P<0.001) and 2.133 (95% CI, 1.689– 2.694; P<0.001), respectively, as shown in Table 2.

Three models of falls and falls resulting in injuries in individuals with benign prostatic hyperplasia compared to those without falls
Subgroup Analysis
In the subgroup analysis, we assessed the influence of BPH on falls, considering visual and auditory impairments, cognitive decline, depression, lower motor weakness, and limitations in daily activities. Notably, individuals with BPH who experienced visual or auditory impairment, cognitive decline, depression, lower motor weakness, or limitations in daily activities exhibited a higher likelihood of having falls compared to individuals without BPH. Figs. 1 and 2 present the odds of experiencing falls and falls resulting in injuries in individuals with BPH compared to those without falls in the presence of morbid conditions. Fig. 3 illustrates the relative prevalence of falls among older adults, categorized by the absence of a morbid condition, the presence of one, and the presence of 2 or more conditions, as previously detailed. The ORs for falls were 1.369 (95% CI, 0.638–2.938), 1.912 (95% CI, 1.356–2.694), and 1.856 (95% CI, 1.455–2.367), and those for falls resulting in injuries were 1.379 (95% CI, 0.553– 3.442), 1.942 (95% CI, 1.265–2.982), and 2.438 (95% CI, 1.826– 3.254), respectively.
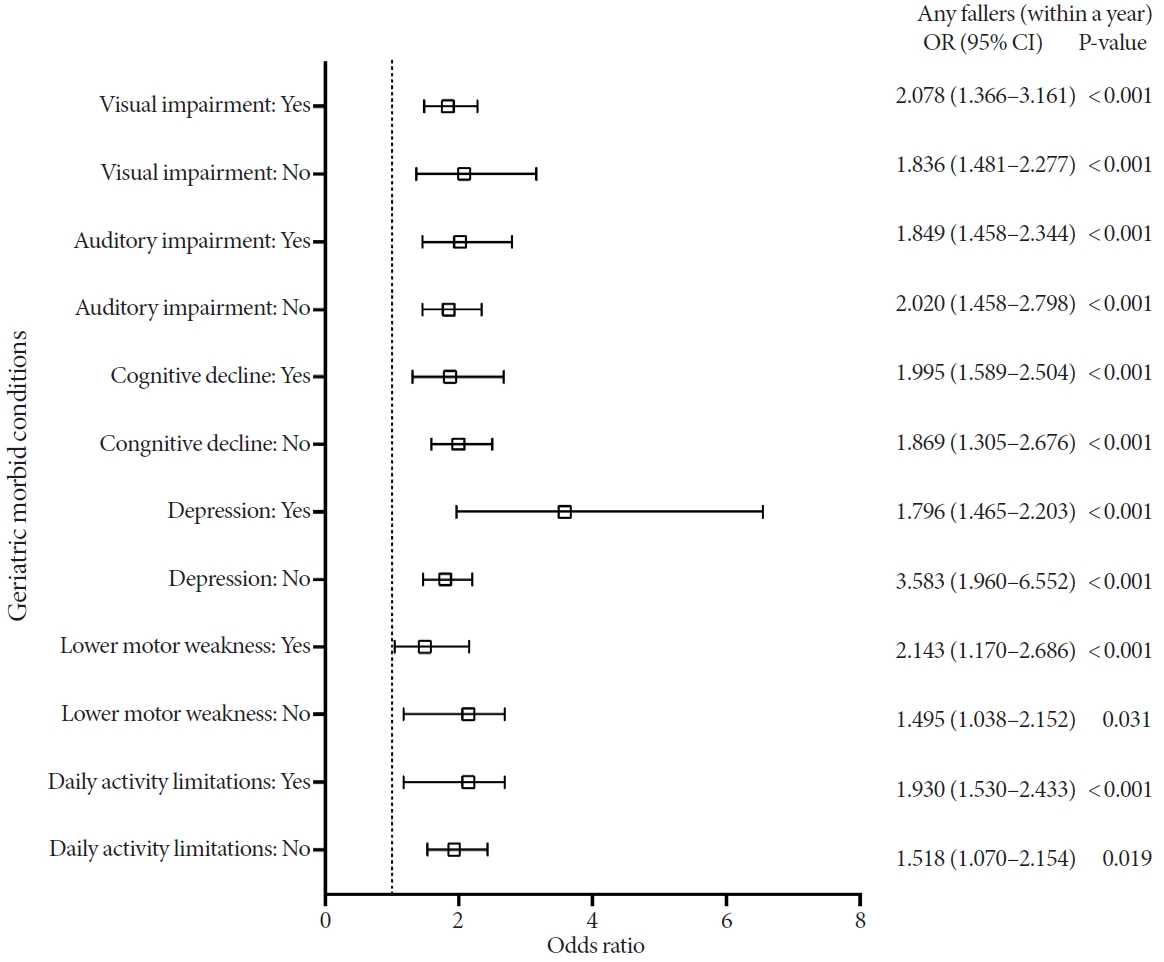
Subgroup analysis of falls in individuals with benign prostatic hyperplasia (BPH) compared to those without falls. Adjusted using model 2, accounting for factors of age, education years, body mass index, total household income, residence area, living pattern, hypertension, dyslipidemia, diabetes mellitus, smoking status, and alcohol consumption. OR, odds ratio; CI, confidence interval.
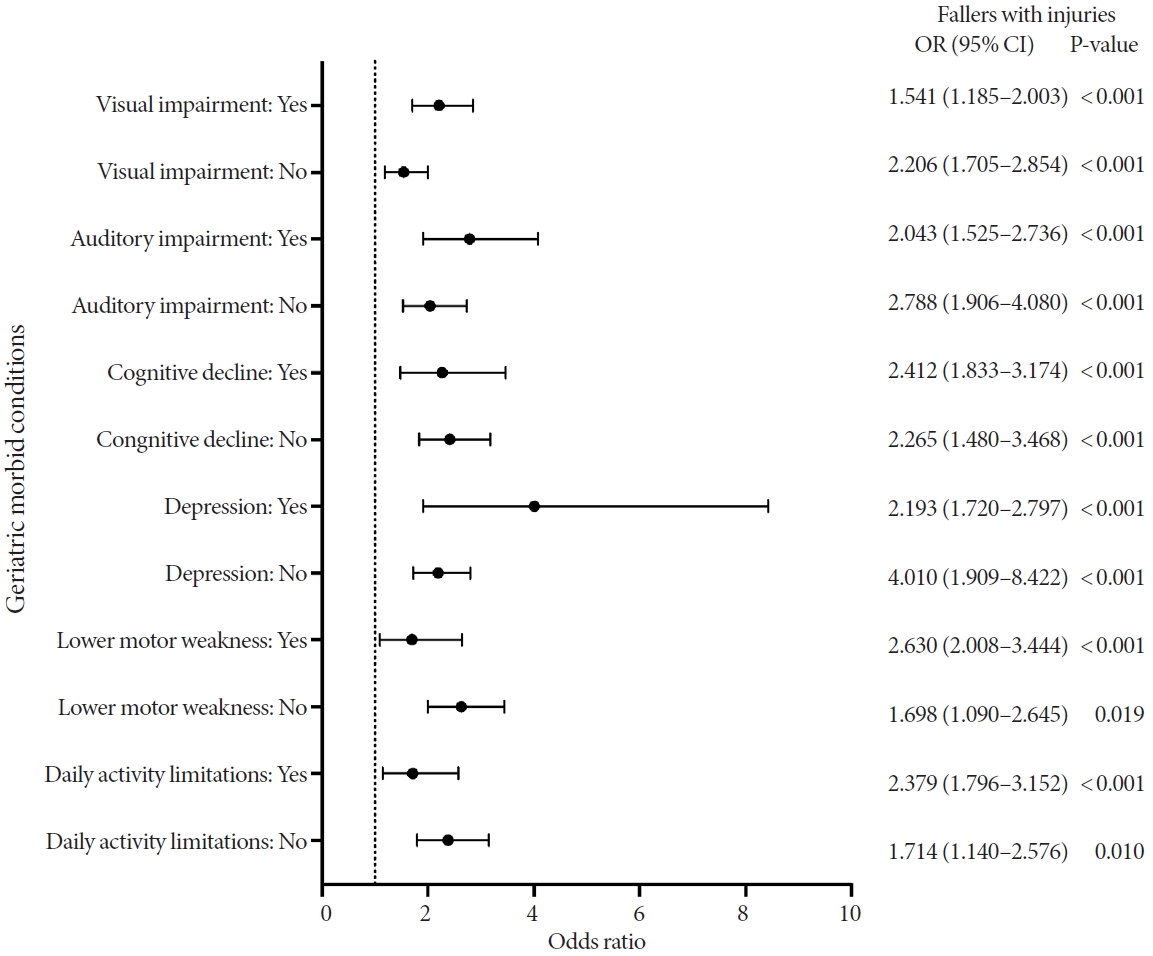
Subgroup analysis of falls resulting in injuries in individuals with benign prostatic hyperplasia (BPH) compared to those without falls. Adjusted using model 2, accounting for factors of age, education years, body mass index, total household income, residence area, living pattern, hypertension, dyslipidemia, diabetes mellitus, smoking status, and alcohol consumption. OR, odd ratio; CI, confidence interval.

Relative prevalence of falls (A) and falls resulting in injuries (B) in individuals with benign prostatic hyperplasia (BPH) categorized by the number of morbid conditions compared to those without falls. Valus are presented as odds ratio (95% confidence interval). Adjusted using model 2, accounting for factors of age, education years, body mass index, total household income, residence area, living pattern, hypertension, dyslipidemia, diabetes mellitus, smoking status, and alcohol consumption. *P<0.05. **P<0.01.
DISCUSSION
The prevalence of BPH shows a consistent upward trend as individuals age, particularly across successive decades [2]. This notable prevalence among older men highlights the importance of this condition, especially in a time characterized by a rapid increase in male life expectancy [2,21,22]. The prevalence of BPH observed in our study was lower than the rates reported in histological studies, suggesting potential underdiagnosis and undertreatment of BPH in the Korean population. Our findings also indicate that individuals with BPH tend to have a range of comorbid chronic conditions and show increased vulnerability to frailty, which is consistent with prior research.
The mechanisms through which BPH contributes to falls are multifactorial. Overactive bladder symptoms, which have been identified as one such factor, cause significant discomfort and are linked to the risk of falls and fractures in both sexes. Urge incontinence, driven by an intense need to urinate, is believed to lead to physical harm due to mobility and balancing problems [11]. Furthermore, nocturia, which involves frequent nighttime urination, heightens the risk of falls due to nighttime walking. Sleep disturbances, leading to daytime drowsiness and fatigue, also cause daytime falls [23]. A meta-analysis revealed that nocturia was associated with an elevated risk for falls (overall relative risk, 1.25; 95% CI, 1.02–1.50), with a more pronounced effect in older individuals [13]. Moreover, the severity of LUTS increases fall risk [10]. For instance, a cohort study involving older individuals who had experienced osteoporotic fractures established that the presence of LUTS, defined as an International Prostate Symptom Score (IPSS) of 8 or higher, was significantly linked to an increased risk of falls [9]. The presence of the aforementioned morbid conditions may exacerbate these risks.
The medications prescribed for BPH are suspected to be another contributing factor to falls. There is growing evidence suggesting that medications such as alpha-adrenergic blockers may induce adverse effects, including low blood pressure, dizziness, and orthostatic hypotension, all of which increase the risk of falls. Furthermore, the overstimulation of the autonomic nervous system due to BPH may also impair gait disturbance, further exacerbating fall risk [24]. Similarly, taking antimuscarinic medications, which are utilized to manage overactive bladder symptoms in BPH patients, is believed to lead cognitive dysfunction, which may contribute to fall risk. However, the assertion that antimuscarinic drugs are a direct cause of falls varies with the type of medication and remains inconsistent depending on the research group and methods [25-27].
The findings of our investigation indicate a significant correlation between BPH and the incidence of falls among the older population. Furthermore, the data suggest that older men with BPH who also have multiple morbid conditions are at an increased risk of falls and related injuries. The survey was conducted on-site, ensuring a complete response rate. The results of this study may be relatively generalizable to older adults as the potential for sample bias is lower than with methods involving online or telephone-based approaches.
Nonetheless, this study had several limitations. The crosssectional study design prohibits the inference of causative relationships from the data. Additionally, while IPSS assessments and uroflowmetry are standard for evaluating LUTS in BPH patients, these were not conducted due to the constraints of the in-person survey methodology. Similarly, transrectal ultrasound, a diagnostic tool for BPH, was not utilized. Future research might use these diagnostic methods to explore the relationship between BPH and fall risk. Moreover, despite efforts to collect data on various morbid conditions that could impact older adults, the study did not account for known risk factors such as balance and grip strength. The study also aimed to assess the severity of falls, yet the specific causes of injuries were not detailed; therefore, subsequent studies should include data on the causes of falls.
In conclusion, our study has demonstrated an increased prevalence of BPH in older adults and its association with falls, particularly among older men and those with underlying morbid conditions. Implementing measures to prevent falls within the geriatric population may benefit these vulnerable individuals. Future research should focus on large-scale, well-designed interventions targeting older individuals under complex morbid conditions.
Notes
Grant/Fund Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Research Ethics
This research was conducted in compliance with applicable laws, regulations, and ethical standards, adhering to the principles outlined in the Declaration of Helsinki and Good Clinical Practice guidelines. The study protocol was approved by the Institutional Review Board (IRB) of Hallym University Kangnam Sacred Heart Hospital (IRB No. HKS 2023-10-017). The requirement for obtaining informed consent was waived by the board.
Conflict of Interest
STC, a member of the Editorial Board of International Neurourology Journal, is the corresponding author of this article. However, he played no role whatsoever in the editorial evaluation of this article or the decision to publish it. No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
· Conceptualization: SJK, STC
· Data curation: SJK
· Formal analysis: SJK
· Methodology: SJK, STC
· Project administration: DL, SGP, SP, YGL, STC
· Visualization: SJK, DL
· Writing - original draft: SJK, STC
· Writing - review & editing: SJK, STC