INTRODUCTION
The "gold standard" of prostate cancer treatment is now open, laparoscopic, or robot assisted laparoscopic prostatectomy with seminal vesiculectomy, and if indicated, staging lymphadenectomy. However, these procedures are not suitable for all patients due to several factors, including their high surgical invasiveness, risk for aged patients and those with comorbidities, and expense. Several alternative treatments, such as high-intensity focused ultrasound (HIFU), transurethral microwave thermotherapy, cryotherapy, and brachytherapy have been developed. However, the existence of a satisfactory alternative method with the potential to achieve complete cancer control was not conclusively proven prior to this study [1-7].
As with open, laparoscopic, or robot assisted laparoscopic prostatectomy, a complete resection of the prostate gland including cancerous tissues can be achieved using total transurethral resection of prostate cancer (TURPC) as an alternative therapy was first recognized by Hans J. Reuter. This can be complemented by simultaneous laparoscopic staging lymphadenectomy and seminal vesiculectomy. Thus, we conducted this study to verify total TURPC with related complications as an alternative therapy for localized prostate cancer.
MATERIALS AND METHODS
The study began in January 2008 and ended in July 2011, approved by Institutional Review Board. A total of 14 patients with a mean age of 76.1 years (range, 66 to 89 years) treated by TURPC were included in this study. Neoadjuvant hormonal therapy was administered in 5 cases to reduce total prostate volume for a shorter operating time. The patients included in this study had proven localized prostate cancer of clinical stage T1-T3a by 2002 American Joint Committee on Cancer tumor, node, metastasis stage, based on histological analysis, preoperative staging by digital rectal examination, International Prostate Symptom Score, maximal flow rate, transrectal ultrasound, prostate-specific antigen (PSA) levels, bone scan, abdomen and pelvic computed tomography (CT), and chest X-ray. Preoperatively detected metastases or treatment by radiotherapy resulted in exclusion from the study. This is a pilot study conducted for the first time in Korea. Therefore, most of the patients were aged over 70 years with or without comorbidity, and thus were not suitable candidates for conventional radical prostatectomy. The patients were stratified into the following 3 risk groups: low risk (clinical stage, T1a-T2a; preoperative PSA level, ≤10 ng/mL; and biopsy Gleason score, ≤6), intermediate risk (clinical stage, T2b-T2c; preoperative PSA level, 10 to 20 ng/mL; and biopsy Gleason score, 7), and high risk (clinical stage, T3a; preoperative PSA level, >20 ng/mL; or biopsy Gleason score, 8 to 10) [8].
We administered prophylactic antibiotics by intravenous injection 30 minutes before surgery. All patients were operated on under spinal or epidural anesthesia. Irrigating fluid level did not exceed 60 cm above the symphysis of the patient in the lithotomy position. Five patients had been receiving neoadjuvant hormonal treatment with bicalutamide and luteinizing hormone releasing hormone. Monopolar transurethral resection of prostate (TURP) was performed with a 26-Fr continuous flow resectoscope (Karl Storz GmbH & Co. KG, Tuttlingen, Germany) using Urosol (CJ, Seoul, Korea). The maximum electrical output of the resectoscope was limited to 140 W for cutting and 80 W for clotting. At the end of the monopolar TURPC, a 22-Fr 3-way urethral Foley catheter with an inflated 50 mL balloon was inserted, and gentle traction was maintained at about 250 g for 4 hours. Continuous saline irrigation was performed until the urine draining from the urethral Foley catheter became clear in the absence of irrigation. Patients were usually discharged on the second postoperative day. The transurethral catheter was removed on the seventh postoperative day in our outpatient department.
Follow-up assessments, with serum PSA testing, rectal examination, and transrectal ultrasound, were given every 3 months in the first and second year, then every 6 months with CT and bone scans once a year for the first 5 years. Subsequent follow-up visits took place once a year.
RESULTS
The 14 patients undergoing total TURPC were aged 66 to 89 years (mean age, 76.1 years). The mean duration of TURPC was 51.7 minutes (range, 30 to 120 minutes), and the mean amount of resected prostatic tissue was 21.2 g (range, 5 to 66 g). The number of patients in each risk group, based on pretreatment PSA level, biopsy Gleason score, and clinical stage (Table 1), were as follows: low risk, 1; intermediate risk, 6; and high risk, 7.
Perioperative complications are listed in Table 2. An intra- and/or postoperative blood transfusion was necessary in 2 cases. Endoscopic examination for bleeding was not required. There was no need in any of the cases to perform open surgery due to complications of the total TURPC. Hyponatremia was found in 7 patients. Bladder neck contracture requiring sound dilatation occurred in 1 case. Incontinence was classified into 3 grades according to the Stamey scale. Six months after TURPC, 3 cases of grade 1, 1 case of grade 2, and 0 cases of grade 3 incontinence were observed.
Three patients in the high-risk group did not achieve a PSA nadir of ≤0.2 ng/mL. The Prostate Cancer Guidelines Panel of the American Urological Association recommend defining biochemical recurrence after radical prostatectomy as an initial serum PSA level of 0.2 ng/mL or greater, with a second confirmatory PSA level greater than 0.2 ng/mL [9]. PSA recurrence occurred in 1 case in our series.
Postoperatively, 7 patients, including the 3 who did not achieve a PSA nadir of ≤0.2 ng/mL and 1 with biochemical recurrence, received adjuvant hormonal therapy. Newly developed lymph node or distant metastases were not observed during the follow-up period.
DISCUSSION
Open, laparoscopic, or robot assisted laparoscopic prostatectomy is unsuitable for many patients, for reasons including age, general high-risk factors, prior prostate surgery, obesity, and socioeconomic factors such as religious restrictions or poverty. Analyses of alternative methods such as HIFU, transurethral microwave thermotherapy, cryotherapy, and brachytherapy have been published, but with follow-up times of <10 years and low case numbers. These assessments were therefore of limited value. A PSA nadir of 0.2 ng/mL can be achieved or not after 6 months. This may not necessarily indicate a radical character of these process [1-7,10].
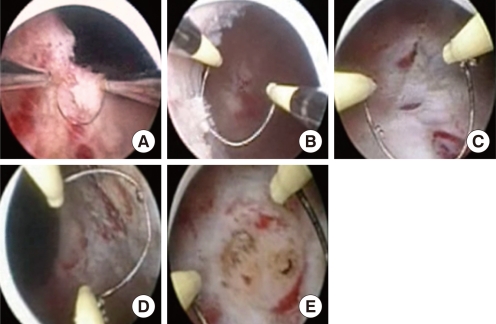
As with conventional surgery, a complete resection of the prostate gland, including cancerous tissues, can be achieved using total TURPC under any circumstances. The boundaries of the prostate capsule, the bladder neck, and the membranous urethra can be identified with the aid of video image magnification (Fig. 1).
Reuter et al. [11,12] performed a laparoscopic staging lymphadenectomy in patients at potential risk of cancer and a life expectancy of >10 years. Patients who have tumors in the preserved seminal vesicle or lymph nodes may not experience a PSA nadir of ≤0.2 ng/mL postoperatively, and will require adjuvant hormonal therapy with or without laparoscopic seminal vesiculectomy or lymphadenectomy. However, we have only given adjuvant hormonal therapy in 3 cases with a PSA nadir >0.2 ng/mL because of aged patients, comorbidities and the refusal of invasive intervention.
For prostate cancer focal therapy, 4 modalities appear to have the most clinical promise: HIFU, cryotherapy, radiation therapy, and photodynamic therapy [13]. If patients with localized prostate cancer are suitable candidates for focal therapy, we can choose the partial TURPC as an alternative procedure. In our experience, we performed right-side TURPC as a focal therapy in a case of prostate cancer confined within the right lateral lobe. Impotence and incontinence are the major side effects of surgical treatment of prostate cancer. This is due to the vulnerability of the nerve plexus and blood vessels supplying the periprostatic tissue, sphincter, and penis [14]. Accordingly, the transurethral approach to the prostate is optimal because the periprostatic tissue, containing the neurovascular bundles, remains intact. The electrical current through the tissue is limited to 140 W for cutting and 80 W for clotting. The tissue is coagulated and cut without the formation of necrosis and with less depth, thus protecting the neurovascular bundle. We reduce the electrical current when applying the resectoscope to the external sphincter muscle.
Irrigation is needed to clarify the surgical field, and since the cutting is done by electricity, the irrigating fluid should be free of electrolytes. However, transurethral resection carries the risk of TUR syndrome caused by irrigation fluid absorption. The increase in dynamic and static pressure increases the risk of fluid absorption, which must be avoided to prevent TUR syndrome and the spread of prostate cancer cells [14,15]. Reuter et al. reported that the key to circumvent such problems is to use low-pressure irrigation with an irrigation fluid level less than 20 cm, and preferably 10 cm above the pubic region using a suprapubic trocar. Thus, the capsule can be resected without being limited by the need for a short surgical time or by prostate weight; the absorption of fluid through capsular perforations is prevented; and blood loss is reduced by a better and more spontaneous control of arterial and venous bleeding [11-15]. TUR syndrome was defined as a serum sodium level of 125 mmol/L or less after TURP with 2 or more symptoms or signs of TUR syndrome, such as nausea, vomiting, bradycardia, hypotension, hypertension, chest pain, mental confusion, anxiety, paresthesia, and visual disturbance. TUR syndrome did not occur, but hyponatremia was seen in 7 cases in our series. This was treated easily using intravenous furosemide injection with or without 3% NaCl solution. Due to inexperience, we used irrigation fluid at 60 cm above the symphysis of the patient without a suprapubic trocar. This may increase fluid absorption into the venous plexus. Our policy was to keep the resection time as short as possible and to not exceed 60 minutes. We consider that a prostate volume of less than 50 mL, as determined by transrectal ultrasound was sufficient to ensure safe, fast operation of this procedure.
Reuter et al. [11,12] conducted a second surgical session at 8 to 12 weeks to reduce the risk of positive margins in the remnants of the prostate, similar to the re-transurethral resection of bladder tumor procedure for bladder cancer. In general, local recurrences can also be resected with a new biopsy as the primary option before radiation or antiandrogen therapy. We did not have a second surgical session in this series. In 3 cases where a PSA nadir of ≤0.2 ng/mL was not achieved until 12 weeks after the operation, adjuvant hormonal therapy was administered because of older age and comorbidity.
Reuter et al. [11,12] performed pathological staging during surgery, taking samples in the following order: the 3 lobes one by one, the verumontanum, the 2 dorsal quadrants of the true capsule (at 6 to 9 and 3 to 6 of the endoscopic clock), the seminal vesicles, the terminal portion of the vas deferens, the prostatic pedicles at 5 and 7, and the 2 ventral quadrants of the capsule (at 9 to 12/12 to 3 of the endoscopic clock). However, we chose not to perform frequent fractional extraction of the tissue in order to speed up operation time. Therefore, the exact histological stages of tumors in this case series could not be shown.
Incontinence is caused by damage to the nerves and/or is a result of a preoperatively existing pelvic floor weakness. A direct violation of the external sphincter muscle is unlikely with careful surgery [14,15]. Although the mean age of patients and the risk of pelvic floor insufficiency were relatively high, the grade 2 incontinence rate 6 months after surgery was only 7.1%. No patient complained of nocturnal incontinence. The risk of erectile impotence was not investigated in this series. A scarred bladder neck is the most common postoperative complication [13,14]. It should be treated by early dilatation with a 24-Fr sound, or an electrical or laser incision. In addition, the urine is alkalinized with citrate to prevent scarring of the bladder neck. The prognosis of bladder neck stricture is usually good. In our case series, it was treated easily using 24-Fr sound dilatation. A PSA nadir of ≤0.2 ng/mL can be achieved in 95% of cases, which is proof of the efficacy of total TURPC [11,12]. The 5-year PSA recurrence rate was 18% for stage pT2 cancer, and the 10-year survival rate was 85% for stage pT3. These results are equivalent to those of similar surgery reported in recent studies [16-30]. PSA recurrence occurred in one case in our series although the short follow-up duration. We examined PSA nadir to predict relapse after TURPC [10]. A PSA nadir of ≤0.2 ng/mL was not achieved in 3 cases of the high risk group. Postoperatively, 7 patients including 3 with a PSA nadir >0.2 ng/mL, and 1 with biochemical recurrence received adjuvant hormonal therapy. Newly developed lymph node or distant metastasis was not observed during the follow-up period.
In conclusion, using total TURPC in all 14 cases in this series, we achieved a complete resection of the prostate gland including cancerous tissues, but excluding the seminal vesicle and lymph nodes, which was comparable to that achieved using other surgical procedures. This is reflected in the PSA nadir, which is in the majority of cases below ≤0.2 ng/mL. TURPC avoids the typical risks of extraprostatic access, because the periprostatic tissue is not severed in order to reach the prostate. Therefore, injury to the nerves in the periprostatic tissue can be avoided, reducing the risk of impotence and incontinence. TURPC is also inexpensive and non-invasive, and requires short hospitalization and a short surgical time without vesicourethral anastomosis.