INTRODUCTION
Nocturia is a common symptom in adult women with pronounced impact on sleep, quality of life and general health [1]. According to the definition of the International Continence Society, nocturia is the complaint that an individual wakes one or more times to void urine at night [2]. Most of the published studies have tendency to focus on nocturia in men, because of the presumed correlation between nocturia and bladder outlet obstruction [3,4], even though nocturia is also common in women [5]. Nocturia becomes increasingly common with increasing age in both men and women [6], and is associated with considerable morbidity and general health. Many number of studies have demonstrated that a high proportion of patients estimating from 63 to 75% with nocturia complaining nocturia to be troublesome symptom [5,6]. Fragmented and disturbed sleep patterns may be observed in patients with nocturia that can result in disturbance of good sleep, daytime sleepiness and serious health risks in the this population [7].
Nocturia is associated with a various conditions and circumstances. Major cause of nocturia fall into three categories that is diurnal polyuria, nocturnal polyuria, and low nocturnal bladder capacity. Nocturia may represent nocturnal frequency from the symptoms of frequent voiding of small volumes, possibly secondary to bladder overactivity and decreased nocturnal bladder capacity, or nocturnal polyuria due to the large amounts of urine production during the night time that may suggests pathology other than from the lower urinary tract [8]. The patients with polyuria experience both increased daytime and night time urinary volume from the increased free water or osmotic dieresis.
Although nocturia is recognized as being common among women, there are limited data on the exact etiology of nocturia and the prevalence of nocturia by age increase in women. The aim of the present study was to evaluate the influence of age on the occurrence of nocturia and type of nocturia and to give a clue in further clinical approach to proper management on nocturia in women.
MATERIALS AND METHODS
Participants
We conducted this study from our female lower urinary tract symptoms (LUTS) database at Chonnam National University Hospital for all patients presenting to our clinic between January 2006 and December 2008. Of 450 total patients, 118 female patients who met the inclusion criteria and complete data are included in this analysis. At initial visits, all patients underwent a detailed clinical evaluation involving complete history taking, physical examination, International Prostate Symptom Score (IPSS) and urinalysis.
Patients were included if they were aged >20 years, had moderate to severe LUTS (IPSS sum >8), and nocturia of at least once per night (IPSS nocturia score of question 7). The subjects with confused or depressed mental status, medication that may alter or control bladder symptoms, symptomatic urinary tract infection, uropathologic condition such as urinary stones and urogenital cancer, pelvic organ prolapsed over stage 3 and neurogenic bladder were not included. The patients with severe symptom of stress urinary incontinence (stamey grade 3), restricted mobility, and night working job were also excluded from this analysis. All patients signed an informed consent agreement.
Frequency Volume Chart
Patients were requested to complete three days frequency volume (FV) charts. They were taught how to complete FV charts precisely by urologist, and asked not to alter their usual fluid intake and voiding habits during the study. The times that arose in the morning and went to bed at night were recorded on the FV charts. Numbers and volumes of voids were estimated by taking a mean over the three day study period. Night time was defined as the time from bedtime to rising in the morning. First morning voided volume was included in the nocturnal urine volume because first morning void is considered to be excreted during sleep and the first morning void was not included in the number of nightly voids. Nocturnal polyuria was defined as a night time urine production of greater than 35% of the daily total volume.
Statistical Analysis
For statistical analysis, patients were stratified by age, those<40 years, 40≤age<60 and those≥60 years. Data were compared statistically using the ANOVA test. A 5% level of significance was established for all of the statistical testing. Statistical analysis was performed using SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
The patient characteristics are listed in Table 1. The mean age was 57.2±11.8 and the mean frequency of nocturnal voiding episodes was 2.7±1.8. The mean duration of symptoms was 26.1±18.6 months. The incidence of hypertention and cardiovascular disease was 15.3% and 4.2%, respectively.
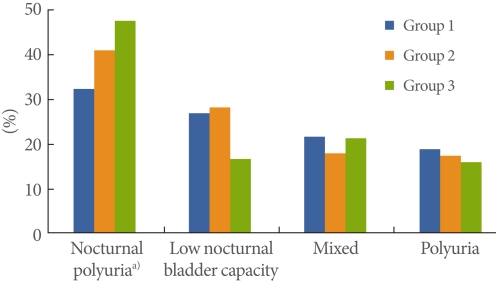
In all age group, noctural polyuria was the major cause for noturia (40.8%), followed by low nocturnal bladder capacity (23.7%), mixed type of nocturnal polyuria and low nocturnal bladder capacity (20.3%) and polyuria (15.2%). Table 2 exhibits the age related change in the cause of nocturia. As a major cause of nocturia, there was a significant increase of the incidence of nocturnal polyuria in aged group: group 1, 32.4%; group 2, 41.0%; group 3, 47.6% (P=0.05). Fig. 1 shows that nocturnal polyuria in the etiology of nocturia is significant increase by age without any significant difference between groups in other caterogry of nocturia; low nocturnal bladder capacity, mixed type and polyuria.
DISCUSSION
In the present study, we evaluated the impact of age on nocturia in women. In overall age group, nocturnal polyuria and decreased nocturnal bladder capacity are the major causes of nocturia in women. Nocturnal polyuria was the major cause of nocturia especially in aged women of 60 years and above. Given the impact of nocturia on general health, nocturia should be routinely assessed by urologic clinicians and should be treated based on the exact cause of the nocturia.
As a clinician, we can easily meet those patients with complaining of restricted social activity, bothersomness and life style change due to bothersome lower urinary symptoms including nocturia. From many studies that have examined the influence of nocturia on general health and quality of life, a high impact has been shown. Truthfully, nocturia has been considered as the most bothersome symptom of lower urinary tract symptoms from the patient and clinical doctor, and there is an association between the extent of impact and the frequency of nocturnal voiding [9,10]. Nocturia has also been associated with an increased risk of falling down in aged people showing a increasing risk of fall down from 10 to 21% with ≥2 micturitions per night as well as limb fracture, excessive daytime somnolence and nocturnal enuresis [11,12]. For the patients with awaking twice or more at night, the reported impairment of health related quality of life was similar to that of Type II diabetes mellitus [13]. In a study especially in working women, the number of days absent from work due to sickness was related to the frequency of night time voiding. Increased well-being was also associated with fewer voids and better sleep quality in women [14,15].
Nocturia or nocturnal micturition is a widespread phenomenon. Given the high prevalence of nocturia among the elderly, nocturia is often viewed as a natural part of aging. However, the incidence of nocturia and the total number of voiding episodes increases with age. Age related physiological changes can alter the regular pattern of urine excretion and lead to an increased nocturnal frequency of voiding. Additionally, aging is associated with anatomical and physiological changes of the urinary tract, which predispose towards increased urinary frequency and urine volume. It is difficult to get a precise figure for the prevalence of nocturia in age peaple, because epidemiological studies have varied in their definition of the condition. Furthermore, there have been relatively few such studies especially in women over the last decade. Coyne et al. [13] conducted a national survey by telephone of 5,204 community-based adults with an average age of 45.8 years, and reported that 31% showed at least one void per night and 14.2% showed at least two voids per night. As an asian study, Yoshimura et al. [16] reported that nocturia found at a rate of 28.5% when nocturia was defined as ≥2 voids per night. In all studies, the prevalence of nocturia was observed to increase dramatically with age [13,17]. Despite a widespread belief that nocturia is more common in men because of the association of nocturia with lower urinary tract symptoms associated with benign prostatic hyperplasia, the incidence of nocturia is in fact similar for men and women [13,16,17]. In a Finnish population reported by Tikkinen et al. [18], the prevalence of nocturia, with a definition of nocturia as having at least one void per night, was 37% and 43% among males and females, respectively. There should be a consideration on, however, little doubt that many older people regard nocturia as an inevitable part of growing, older people could thus underreport the extent of the nocturia and realted lower urinary tract symptoms as a problem.
In addition to the age related physiological changes to lower urinary tract function, nocturia in elderly appears to have a higher daily urine production than age matched controls without nocturia. These individuals also produce a higher proportion of their daily urine output at night [19]. There has been suggested that this physiological changes which might lead to an older adult experiencing an increased nocturnal urinary frequency [20], and the reduction in functional bladder capacity and reduced sensation of bladder filling associated with later life. This reduction in functional bladder capacity may be related to the alteration in collagen to smooth muscle ratio seen in aged people [21]. In the present study, we found out the consistent result in terms of the usual cause of nocturia, nocturnal polyuria and decreased nocturnal bladder capacity are the most common causes of female nocturia. Also we report that nocturnal polyuria was the major cause of nocturia with in aged women. Nocturnal polyuria and decreased nocturnal bladder capacity should be considered in aged female with nocturia and sould be treated based on the indivisual exact cause of nocturia.
Sleep disturbance leading to waking, drinking during the waking period and spend excessive amounts of time in bed may account for the nocturia as well. Many older people tend to have their drinking habits including fluid intake late at night including alcohol [22]. Other causes such as controlled diabetes mellitus, heart failure can induce polyuria due to raised artrial natriuretic peptide levels and an increased non-osmotic drive to thirst, hypercalcemia though perhaps becoming more common due to the increased prevalence of oral calcium supplementation, dependent edema due to venous stasis or hypoalbuminemia, diuretic late in the day that may lead to dependent ankle edema are suggested [23]. Nocturia has also been associated with obstructive sleep apnea, related to elevated night time urine production and atrial natriuretic peptide excretion in response to cardiac distension caused by negative pressure within the chest. Therefore the usual pattern of fluid intake and drinking habit such as alcohol consumption should be ascertained. A detailed drug history, looking for the use of medication which might predispose to nocturnal voiding or timing of medication such as diuretics and antihypertensive medication should be taken together and should give an exact counsel to make an alteration if possible. When nocturia is present, clinicians should try to identify its exact causes by exclude significant lower urinary tract pathology and associated disease. Once the specific cause or causes are found, most cases can be satisfactorily managed using specific management strategy based on the specific cause of nocturia [24].
This study has some limitations and should be pointed out with regard to the study design. First, this study is cross sectional study and subject to recall bias. Many important variables in this analysis such as comorbid conditions, medications can affect bladder condition and nocturia, are based on entirely on participant reports without clinical verification. We used FV chart in three days. FV charts are widely used by clinicians interested in voiding dysfunction. These charts have many advantages of representing themselves the exact daily habits of voiding easily at home. In this study, we were not able to check the amount of water drunk by our patients, which record voided volume and the time of each micturition, day and night. In addition, we excluded those women with stress incontinence and restricted mobility that can also have an impact on the nocturnal frequency. Nevertheless, this descriptive analysis provides additional insight on the impact of age on the nocturia and the major cause of nocturia in aged women. Given the finding of this study, the importance of further evaluation of nocturia and treatment base on the exact cause of nocturia of women in clinical setting should be reminded.
In conclusion, the frequency of nocturnal voiding episodes change with age in women. In most cases, nocturia was caused by nocturnal polyuria and decreased nocturnal bladder capacity. Nocturnal polyuria was the major cause of nocturia with age over 60 years old. Nocturia could be classified and treated based on these results.