INTRODUCTION
The Q-tip test is a long-standing urogynecological examination, first developed by Crystle et al. in 1971 [1]. It is a simple and objective method to measure urethral hypermobility in women with stress urinary incontinence (SUI). The Q-tip test has been used to predict the surgical outcomes of anti-incontinence surgery. In general [2-4], the Q-tip test has high test-retest reliability [5]. However, some factors, such as patient position, bladder filling state, and anterior vaginal wall relaxation, may affect the reliability of the Q-tip test [6,7].
During the Q-tip test, a cotton swab is inserted into the urethra, which may result in urethral discomfort [8]. However, the Q-tip test still plays an important role in predicting the outcome of anti-incontinence surgery. A higher Q-tip angle has been reported to be associated with higher success rates of midurethral sling procedures [2-4]. Thus, identifying clinical or urodynamic factors that affect the Q-tip angle would facilitate more accurate interpretations of the results of the Q-tip test, enabling more informed preoperative consultations and better prediction of postoperative outcomes. Therefore, the main objective of this study was to identify clinical and urodynamic predictors of the Q-tip angle.
MATERIALS AND METHODS
Between January 2014 and June 2019, all women with lower urinary tract symptoms who underwent Q-tip testing, pad testing, and urodynamic studies were included in this retrospective study. The short form of the Urinary Distress Inventory (UDI) questionnaire, the short form of the Incontinence Impact Questionnaire (IIQ), bladder diaries, and the degree of pelvic organ prolapse were reviewed from the patients’ medical records. The degree of pelvic organ prolapse was determined using the Pelvic Organ Prolapse Quantification system [9]. This study was approved by the research ethics committee of the hospital.
The Q-tip test was performed with the patient in the supine lithotomy position during a pelvic examination at our outpatient clinic. A sterile, lubricated cotton swab was inserted into the urethra to the level of the bladder neck, and the axis change with straining was then measured with a goniometer. The Q-tip angle was defined as the angle at maximum straining as measured from the horizontal plane [10]. A Q-tip angle ≥30° was defined as indicating urethral hypermobility.
With each patient in a seated position, urodynamic studies were performed using a Life-Tech 6-channel monitor with computer analysis and the Urolab/Urovision System V (Life-Tech, Inc., Houston, TX, USA). The urodynamic studies included uroflowmetry, filling cystometry with 35°C distilled water at a rate of 60 mL/sec, a pressure flow study, and a stress urethral pressure profile with a strong-desire volume of distilled water in the bladder [11]. Additionally, a 20-minute pad test was performed for each woman [12].
Urodynamic stress incontinence (USI) was diagnosed when involuntary urine leakage occurred during filling cystometry and was associated with increased intra-abdominal pressure in the absence of a detrusor contraction [9]. Patients who had a strong desire to void at a volume of less than 300 mL were considered to have bladder oversensitivity [13]. Detrusor overactivity (DO) was defined as evidence of spontaneous detrusor contractions occurring during bladder filling or an uninhibited detrusor contraction occurring at a cystometric capacity that usually resulted in voiding [14]. Functional bladder outlet obstruction was evidenced by uroflowmetry results of a maximum flow rate (Qmax) of <12 mL/sec and a detrusor pressure at Qmax of >40 cm H2O measured via voiding cystometry without a known anatomic cause of obstruction [15]. The pressure transmission ratio (PTR) was defined as the increment in urethral pressure upon coughing as a percentage of the simultaneously-reported increment in vesical pressure [10]. In this study, the PTR at maximum urethral pressure (MUP) referred to the PTR measured near or at MUP [16].
All terminology used in this paper conforms to the standards recommended by the joint report published by the International Urogynecological Association and the International Continence Society [9]. All procedures were performed by an experienced technician, and the data were interpreted by a single observer to avoid interobserver variability.
STATA ver. 11.0 (Stata Corp., College Station, TX, USA) was used for statistical analysis. To identify predictors of the Q-tip angle, multivariable backward stepwise linear regression analysis was performed for all variables that showed a significant correlation using the Spearman rank correlation coefficient. A P-value <0.05 was considered to indicate statistical significance.
RESULTS
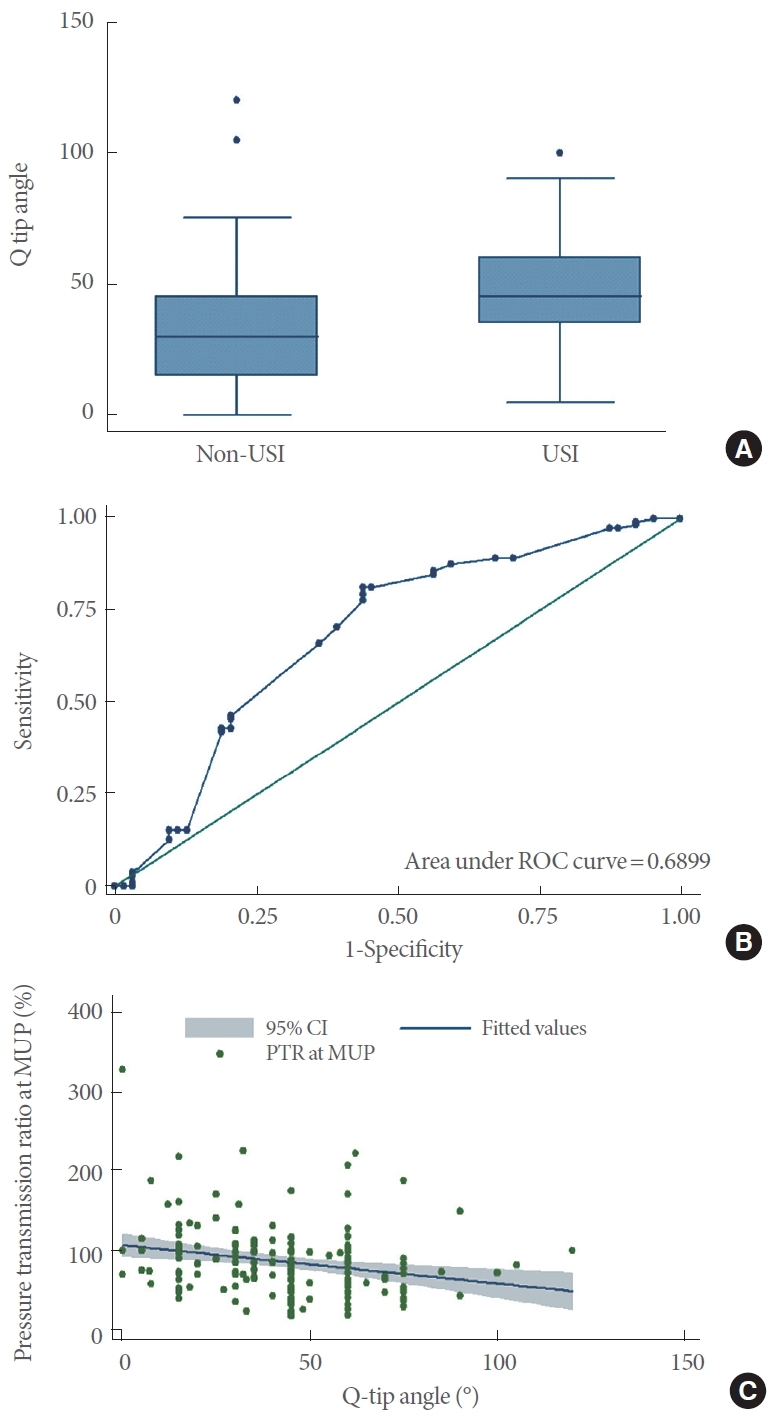
The records of a total of 176 women were reviewed in this study (Table 1). The average Q-tip angle was 43.1°±22.5°. The Q-tip angle differed between women with and without USI (48.0°±19.7° vs. 34.5°±24.6°, respectively; P<0.0001) (Fig. 1A). Based on a receiver operating characteristic curve (ROC) analysis, the optimum Q-tip angle for the prediction of USI was ≥32°, and this cutoff had an area under the ROC curve of 0.69 (95% confidence interval [CI], 0.60–0.78; sensitivity, 81.3%; specificity, 56.3%; Fig. 1B).
We assessed the correlations between the Q-tip angle and clinical and urodynamic parameters, with results shown in Table 2. Age, parity, point Aa, point Ba, point C, SUI, overactive bladder syndrome, voiding dysfunction, USI, DO, pad weight, Qmax, voided volume, PTR at MUP, the score on the third question of the UDI questionnaire (“Urine leakage related to physical activity, coughing or sneezing?”), and the score on the fifth question of the IIQ questionnaire (IIQQ5, “Has urine leakage affected your participation in social activities outside your home?”) were significantly correlated with the Q-tip angle (Table 2).
Multivariable backward stepwise linear regression revealed that only age, point Ba, USI, Qmax, PTR at MUP, and IIQQ5 were independent predictors of the Q-tip angle (Table 3).
Univariate regression analysis with the Q-tip angle showed that the regression coefficient of PTR at MUP was -0.12 (95% CI, -0.20 to -0.05; P=0.001) (Fig. 1C), with a constant of 53.8 (95% CI, 46.6–60.9; P<0.001). Thus, the predicted Q-tip angle for a given PTR at MUP (%, a) could be calculated using the following formula:
Q-tip angle=53.8-0.12×a (R2=0.06).
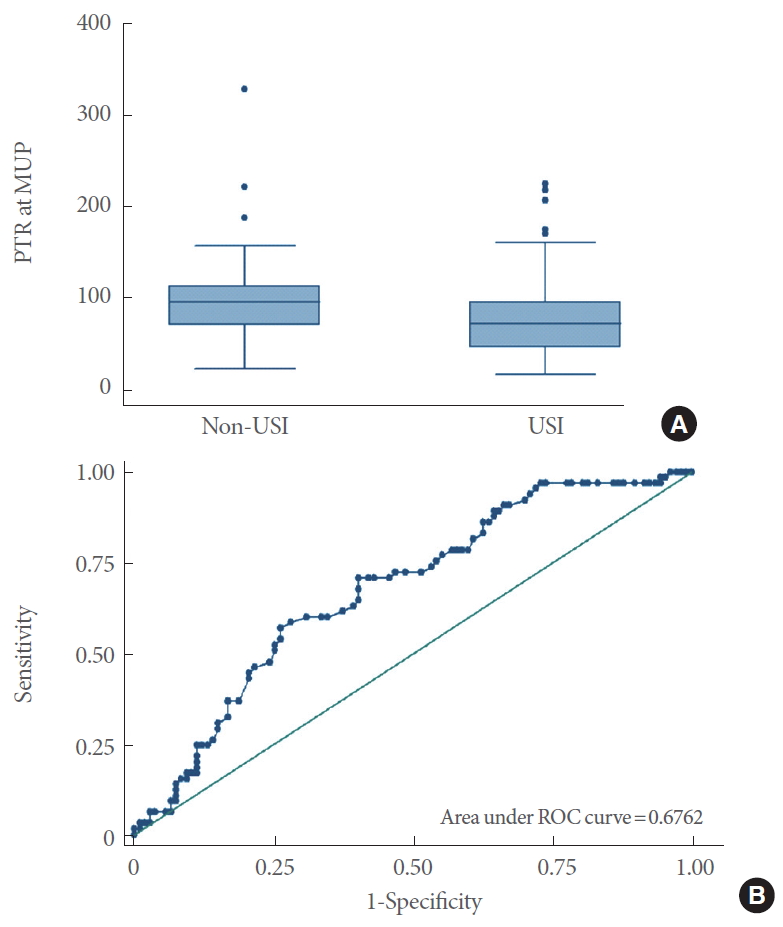
PTR at MUP significantly differed between women with and without USI (77.1%±41.2% vs. 100.0%±46.4%, respectively; P=0.0001) (Fig. 2A). Based on the ROC analysis, for the prediction of USI, the optimum cutoff of PTR at MUP was <81%, with an area under the ROC curve of 0.70 (95% CI, 0.62–0.78; sensitivity, 70.8%; specificity, 59.8%) (Fig. 2B).
DISCUSSION
In this study, we successfully identified PTR at MUP as a predictor of the Q-tip angle. To our knowledge, this is the first article to demonstrate an association between these variables (Fig. 1C). However, only a fair correlation was found between PTR at MUP and the Q-tip angle (Spearman ρ=-0.28, Table 2); thus, PTR at MUP was not found to be an effective surrogate for the Q-tip test (Fig. 2B).
While urodynamic studies are not helpful for determining the surgical outcomes of uncomplicated SUI cases [17], these studies can be used to assess complicated cases. The urethral pressure profile is a component of urodynamic studies. Because PTR at MUP was significantly correlated with the Q-tip angle (ρ=-0.28) (Fig. 1C), a urethral pressure profile study might be performed with stress (i.e., coughing) to obtain PTR data, especially for women with SUI who do not undergo Q-tip testing. An increase in PTR at MUP has been reported as an important finding associated with the resolution of USI after midurethral surgery [16].
In the present study, point Ba was significantly correlated with the Q-tip angle (ρ=0.34; regression coefficient, 4.5; Tables 2 and 3), and point Ba was strongly correlated with point Aa (ρ=0.998, P<0.0001). Similarly, Zyczynski et al. [18] found a moderate correlation between point Aa and the Q-tip angle (r=0.35, P<0.001). Cogan et al. [19] also found that urethral hypermobility was present in ≥95% of patients with stage II or higher anterior compartment prolapse. Additionally, Walters et al. [20] reported that anterior vaginal relaxation was positively associated with the Q-tip angle (r=0.34, P=0.001).
In this study, Qmax (regression coefficient, 0.13) was found to be a predictor of the Q-tip angle (Table 3). We did not find any previous report with similar findings, and the underlying mechanism is unknown. However, owing to the presence of only a fair correlation (ρ=0.28, P=0.0001) (Table 2), Qmax is not an effective surrogate for the Q-tip test.
Age was found to be negatively correlated with the Q-tip angle in this study (ρ=-0.38, P<0.0001) (Table 2) (regression coefficient, -0.55; P<0.001) (Table 3). The underlying mechanism is unknown; however, the strength of abdominal straining may decrease in older women, which might explain the correlation between age and the Q-tip angle. It is worth mentioning that age was found to be positively correlated with the Q-tip angle (r=0.27, P<0.05) by Walters et al. [20].
IIQQ5 asks “Has urine leakage affected your participation in social activities outside your home?”. In this study, IIQQ5 score (range, 0–3) was an independent predictor of the Q-tip angle (regression coefficient, -4.1). The underlying mechanism of this relationship is unknown. However, a positive correlation was found between IIQQ5 and the presence of overactive bladder syndrome (ρ=0.31, P=0.0001) and incontinence episodes (ρ= 0.32, P=0.01), but not SUI (ρ=-0.02, P=0.77) or USI (ρ= 0.07, P=0.39). The above findings may indicate that female patients with overactive bladder syndrome and urgency incontinence have a smaller Q-tip angle (regression coefficient, -4.1).
Because urethral discomfort can occur during Q-tip testing, some authors have tried to substitute it with other surrogates [21-24]. Meyer et al. [21] used a vaginal swab test to predict urethral hypermobility; however, 11 of 80 results (13.8%) were found to be false negatives. Robinson et al. [22] used a visual urethral mobility exam to predict urethral hypermobility; however, the visual urethral mobility exam only contains binomial data (i.e., the presence or absence of urethral hypermobility), not continuous data. In contrast, the Q-tip angle is a continuous variable. A higher Q-tip angle has been reported to be associated with a higher success rate of midurethral sling surgery [2-4]; thus, owing to its binomial nature, a visual urethral mobility exam may not be as effective as the Q-tip test in predicting surgical outcomes. In addition, sonography-derived bladder neck movement has been used to assess urethral hypermobility [23]; however, poor interobserver correlation of sonography-derived bladder neck movement (r=0.43) was found compared with the interobserver correlation of the Q-tip test (r=0.83) [24].
In this study, the cough stress test was performed before the Q-tip test during the pelvic examination. Thus, our patients were asked to have some urine in the bladder before the cough stress test, especially in the cases of women with involuntary urine leakage. Therefore, most Q-tip tests were performed while the patient had some urine in the bladder (i.e., the bladder filling state). Nonetheless, it is worth mentioning that, in the supine position, the bladder filling state was reported to be associated with a higher Q-tip angle than the emptying state (15.4°±9.7° vs. 14.1°±9.1°, respectively; P=0.049) [6].
The limitations of this study include its retrospective nature. However, the optimal Q-tip angle of ≥32° for the prediction of USI in our results is similar to the conventional Q-tip angle of >30° for predicting urethral hypermobility. In addition, detailed data from a pelvic examination, urodynamic studies, questionnaires, and a 3-day bladder diary were reviewed in this study, which may make our data more reliable.
In conclusions, age, point Ba, USI, Qmax, PTR at MUP, and IIQQ5 were found to be independent predictors of the Q-tip angle. However, none of these can serve as effective surrogates for the Q-tip test due to their lack of a sufficient correlation.